Author : Emile R. Mohler, M.D.
Director, Vascular Medicine University of Pennsylvania health system
Penn Web Site: http://www.uphs.upenn.edu/cardio/faculty/mohler.html
Introduction
Carotid
disease is a vascular disorder of the arteries in the neck that carry
blood to the brain. The most common problem that develops in the
carotid artery is a cholesterol plaque. Rarely, the carotid arteries
can tear, resulting in a carotid dissection.
Carotid artery anatomy

The
carotid arteries are medium sized arteries that originate from the
aorta, the main blood vessel that emanates from the left side of the
heart (Figure 1). On the right side, the carotid forms from the
innominate artery off the aorta whereas on the left it arises directly
from the arch of the aorta. The vertebral arteries (Figure 1) also
carry blood to the brain and arise in the back of the neck from a neck
artery called the subclavian.
What is a carotid plaque and how does it develop?
The
carotid artery has three layers – the intima, the media, and the
adventitia. The layer closest to blood flow is the intima (Figure 2).
The arterial wall becomes thickened when cholesterol builds up in the
intima and may protrude into flowing blood. This thickened area of the
artery is called a plaque. Atherosclerosis is the medical term used to
describe the buildup of cholesterol and fibrotic tissue in the arterial
wall. The lining of an artery releases molecules that keep blood moving
and inhibit a blood clot from forming. However, an atherosclerotic
plaque may rupture or ulcerate causing development of blood clot in the
carotid artery.
 The
most frequent cause of a blood clot travelling to the brain from the
carotid is an atherosclerotic plaque. Plaques also contain white cells
called macrophages that absorb the cholesterol. The development of
carotid atherosclerotic plaque results from both genetic and
environmental influences (see below for causes). Patients with carotid
stenosis (narrowing) are at higher risk for an ischemic stroke. Other
more rare conditions that do not involve cholesterol such as
fibromuscular dysplasia and vasculitis may produce carotid blockage.
The
most frequent cause of a blood clot travelling to the brain from the
carotid is an atherosclerotic plaque. Plaques also contain white cells
called macrophages that absorb the cholesterol. The development of
carotid atherosclerotic plaque results from both genetic and
environmental influences (see below for causes). Patients with carotid
stenosis (narrowing) are at higher risk for an ischemic stroke. Other
more rare conditions that do not involve cholesterol such as
fibromuscular dysplasia and vasculitis may produce carotid blockage.How does a stroke result from a carotid plaque?
A stroke, also known as a cerebrovascular accident,
is a term that describes a problem within the vascular system in the
brain that may cause permanent damage. There are two types of stroke,
one where the blood supply is blocked, called an ischemic stroke, and
the other is bleeding into the brain, called a hemorrhagic stroke.
There are approximately 750,000 strokes in the United States per year.
A
stroke due to carotid disease results when a blood clot forms on the
cholesterol filled plaque. The clot breaks off and then travels from the
carotid artery up into the middle cerebral artery, a major supplier of
blood to the brain, and blocks blood flow. The resulting diminished
blood flow deprives the brain of oxygen which results in brain cell
death. Ischemic stroke may manifest as paralysis, slurred speech, or
other neurological problems.
Are some plaques more dangerous than others?
Studies
indicate that plaques with high cholesterol and high white cell content
are more dangerous than plaques which are highly calcified. One study
examined plaques after surgical removal and reported that the plaques
that were filled with sheets of calcium, and even bone, were less likely
to cause a stroke.1 It is thought that the heavily calcified plaques are less likely to rupture and develop a blood clot.
How is carotid disease diagnosed?
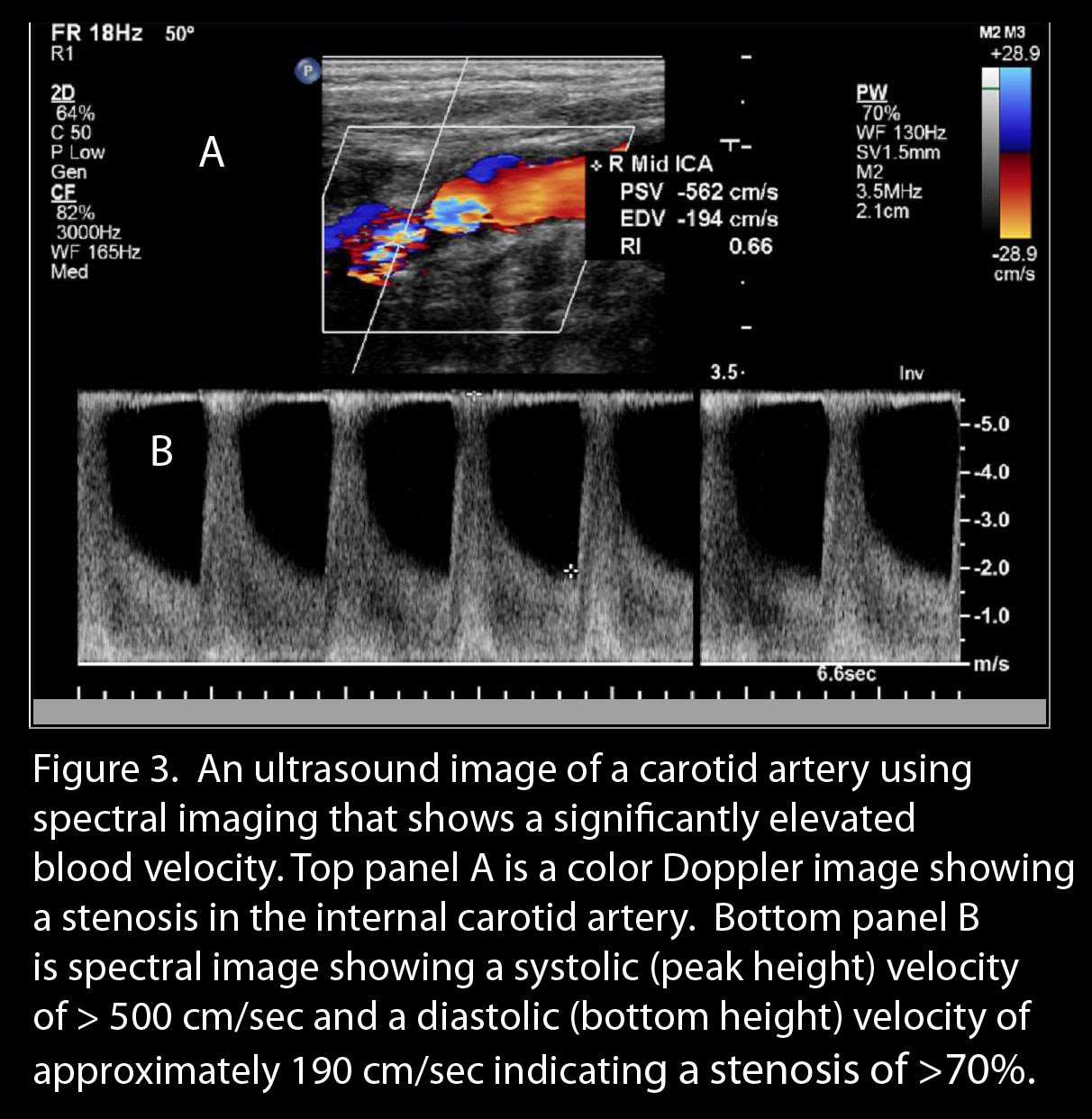
The
initial study to evaluate carotid disease is a carotid ultrasound.
This technique utilizes sound waves to view the carotid artery. A small
amount of saline gel is placed on the neck and an ultrasound probe is
used to visualize the carotid arteries (Figure 3). Ultrasound images
may reveal plaque. The amount of blockage (stenosis in medical
terminology) is determined by the velocity of blood flow through the
artery; the higher the velocity, the higher the amount of stenosis or
narrowing. One ultrasound-based technique evaluates the thickness of
the carotid artery to determine if there is increased risk for stroke or
heart attack (Figure 4). http://www.youtube.com/watch?v=AdbCTjlYZy4The
carotid artery intimal and medial layer thickness is measured, so
called IMT, and a value generated and compared to individuals of similar
age.2 http://www.youtube.com/watch?v=AdbCTjlYZy4A carotid IMT value of > 1mm is considered high risk at any age.
What are the risk factors for carotid disease?
The
major non-modifiable risk factors for ischemic stroke include: age,
inherited pre-disposition, sex, and race (more common in men and in
African Americans). The modifiable risk factors include: hypertension,
diabetes mellitus, cigarette smoking, elevated homocysteine, and
cholesterol (especially in hypertensives).
What is the treatment for carotid disease?
The
treatment for carotid atherosclerotic disease includes medical
intervention (management of atherosclerotic risk factors, antiplatelet
medication) and revascularization (opening the artery) for appropriate
candidates.
What medications are available to treat carotid disease?
In
the late 1980s to the mid 1990s when most of the carotid surgery
studies were being done, the best medical therapy was aspirin. Since
then, new cholesterol lowering drugs and blood pressure control drugs
have been developed that favorably impact on the carotid disease
process.
High Blood Pressure Medication
High
blood pressure is a known risk factor for a stroke, as approximately
60% of strokes are attributed to hypertension. Blood pressure control
is extremely important to prevent strokes. One study called the
Systolic Hypertension in the Elderly Program (SHEP) evaluated blood
pressure control in patients over age 60 years.3
When compared with a placebo (inactive pill), there was a 36% reduction
in stroke incidence over 4.5 years of follow-up with medication.
Antiplatelet Medication
A
blood clot in the carotid artery is formed in part due to an
aggregation of platelets on top of the atherosclerotic plaque. The
first-line treatment of stroke prevention in those who have had a stroke
is antiplatelet medicine such as aspirin, clopidogrel (Plavix), or the
combination of dipyridamole and aspirin (Aggrenox). The data from an
analysis of multiple antiplatelet studies indicate that the risk of a
second stroke decreases by approximately 25%.4
These
drugs act by blocking platelets from adhering and reduce the risk of a
carotid thrombus (clot). The data regarding treatment with an
antiplatelet agent to prevent a stroke from occurring in those who never
had a stroke is not as strong. There are high-risk groups such as
those with diabetes mellitus who will likely benefit from antiplatelet
drug to prevent stroke.
Cholesterol Lowering Medication
High
blood pressure is more of a risk factor for a stroke than high
cholesterol, but recent data indicate that lowering high cholesterol
reduces progression of carotid plaque and stroke.5 The
SPARCL study used an HMG CoA reductase inhibitor (statin drug) to lower
cholesterol and compared it with placebo in those with a stroke or
mini-stroke (transient ischemic attack).6 After a follow-up
of 4.9 years, the statin group had reduced incidence of fatal or
nonfatal stroke. Interestingly, the statin group also had a reduction
in heart attacks.
What is the surgical treatment for carotid disease?
The
surgical treatment for severe carotid disease is removal of the plaque
by a carotid endarterectomy. The surgical removal of an atherosclerotic
plaque has been proven safe and effective in numerous randomized
clinical studies for symptomatic patients (Table 1).
|
Table 1. Amount of Stenosis and Benefit from Surgery
| |
|
Percent of Stenosis
|
Benefit of Endarterectomy
|
|
70% Stenosis or greater
|
Significant
|
|
50-69% Stenosis
|
Marginal
|
|
50% Stenosis or less
|
None
|
Endarterectomy in asymptomatic individuals
Large
clinical trials evaluating asymptomatic patients with carotid
atherosclerosis and ≥ 60% stenosis, such as the Asymptomatic Carotid
Atherosclerotic Study (ACAS), found a risk reduction of 50% over five
years with carotid surgery compared with medical therapy with drugs.
The benefit of carotid endarterectomy was realized approximately two
years after surgery. This result was obtained with a very low surgical
complication rate of 2.3%, half of which were due to cerebral
angiography (contrast dye injection into the arteries of the brain). A
higher surgical complication rate that includes stroke, infection, and
reocclusion of the artery, will delay the realized benefit from an
endarterectomy. Asymptomatic patients with ≥80% carotid stenosis are
likely to benefit from surgery if their life expectancy is five years
and if the operating surgeon has a post-operative complication rate less
than 3%. Of note, current data indicate that the benefit of carotid
endarterectomy in asymptomatic patients is lower in woman compared with
men.
What are the complications of carotid surgery?
Potential
complications associated with vascular surgery include stroke, nerve
damage, and infection. Symptomatic patients have a higher
post-operative complication rate than asymptomatic patients. Some
patients may re-occlude the artery due to scar tissue, so called
recurrent carotid artery disease. The rate of repeat surgery for
recurrent carotid artery stenosis after endarterectomy has been under
10%. For patients who underwent a repair of the carotid artery with a
vein or patch graft, the recurrent stroke rate is under 2% for
individuals with greater than 70% stenosis. In one study, asymptomatic
patients did not benefit from endarterectomy if they had a completely
occluded carotid artery on the opposite side of the neck.
Percutaneous carotid revascularization (Angioplasty & Stenting)
There
are two types of operations, the traditional one using a scalpel, and a
relatively more recent technique where a puncture is done through the
skin with a needle called a percutaneous approach. In this latter
method, a catheter (plastic tube) is inserted through the needle and
into the artery being treated. Percutaneous carotid artery
revascularization has emerged as an alternative therapy to surgical
carotid endarterectomy for the treatment of carotid stenosis.8 The percutaneous approach is attractive given that it is a less-invasive approach that may not have the complications associated with surgical treatment.
The
first percutaneous method developed to treat artery blockages involves
passing a catheter with a balloon attached into the artery and inflating
the balloon to squeeze the plaque against the wall and open the
vessel. Carotid artery balloon angioplasty was first performed in 1979
and a clinical study of carotid angioplasty (CAVATAS) showed, at three
years, there was no difference in the rate of stroke compared with surgery.9
However, percutaneous procedures are not without risk. Catheter
manipulation is associated with death and complications which include
the potential for dislodging a plaque during the procedure resulting in
embolic stroke.
The
early studies of percutaneous carotid angioplasty were directed at
lesions with lower risk of embolic complications, such as early carotid
restenosis and fibromuscular dysplasia. The stroke rates attributed to
the procedure range from 1.4 to 12%. During long-term follow-up,
restenosis of the internal carotid artery is reported to occur in up to
15% of patients and dissection in 5% of patients.
A
second percutaneous method involves placing a metallic stent in the
artery after the balloon angioplasty, in order to keep the artery open.
A carotid stent is preferred to angioplasty, as it can reduce the risk
of threatened vessel closure due to a dissection and, over the
long-term, restenosis. Newer stents are coated with medication to
further reduce the risk of carotid restenosis. Of note, there are
ongoing clinical trials to evaluate if the benefit of a lower restenosis
rate is not offset by later clotting in the artery.
Comparison of percutaneous versus surgical carotid revascularization
Clinical
trials comparing angioplasty and stenting with carotid endarterectomy
have yielded insight into both the success rate and complication rate of
both procedures. There is conflicting data on the efficacy of
angioplasty and stenting compared with endarterectomy. Two initial
trials that did not use embolic protection (see below) indicated a worse
outcome with the percutaneous technique. One such study, the WALLSTENT
Study, showed a one-year, ipsilateral stroke rate higher in the
percutaneous group compared with surgery (12.2% versus 3.6%). Other
trials, such as the Carotid and Vertebral Artery Transluminal
Angioplasty Study (CAVATAS) and a separate randomized trial in a
community hospital found that both treatments had similar major risks
and effectiveness.
Carotid protection devices against stroke
In
order to reduce complication rates from carotid angioplasty and
stenting, protection devices were developed to reduce embolic debris
traveling to the brain. The complication that is trying to be avoided
is dislodging of small bits of plaque lining the blood vessel during the
procedure which could travel in the blood stream and lodge in a brain
artery causing a stroke. Filtering devices or “damming” devices are
temporarily inserted either immediately at the procedure site, or
somewhat upstream to catch the debris and filter it out of the body-
Each of these approaches had some disadvantages but these protection
devices clearly reduce complication rates.
Clinical Trials using embolic protection devices
A
large trial employing distal protection to evaluate against
complicating stroke was the Stenting and Angioplasty with Protection in
Patients at High Risk for Endarterectomy (SAPPHIRE).10 High-risk patients were defined as having at least one of the following:
· Contralateral carotid artery occlusion
· Radiation therapy to the neck
· Previous carotid endarterectomy with recurrent stenosis
· Difficult surgical access, contralateral laryngeal nerve palsy
· Severe multiple lesions in the carotid artery
· Heart failure
· Coronary artery bypass grafting or open heart surgery within 6 months
· Myocardial infarction (heart attack) 1 day to 4 weeks prior
· Angina (chest pain from blocked heart artery) at low work load or unstable angina
· Severe pulmonary disease
· Age greater than eighty years
A
total of 334 patients who had either a symptomatic carotid-artery
stenosis of ≥ 50 % or an asymptomatic stenosis of at least 80 % were
treated with carotid-artery stenting or surgical endarterectomy.11
The primary end-point of the study was death, stroke, or heart attack
after the intervention, which occurred in 20 patients randomly assigned
to undergo carotid artery stenting and in 32 patients randomly assigned
to undergo endarterectomy. Both of the groups in the SAPPHIRE Study had
a relatively high risk of complications at 30 days, which exceeded the ≤
3% recommended as the maximum rate according the American Heart
Association guidelines.12 Other trials are underway to further define the benefit and risk of percutaneous versus surgical carotid revascularization. The Food and Drug Administration has approved a coronary stent for use in carotid arteries.
Potential complications due to carotid stenting include: bradycardia (slowed heart rate), hypotension (low blood pressure), and minor or major stroke. Hyperperfusion syndrome is a relatively uncommon secondary result of carotid endarterectomy, which manifests as headache on the same side as the revascularized artery and may be accompanied by focal seizures and intracerebral hemorrhage. There are few data regarding prevalence of hyperperfusion syndrome after carotid stenting.
Who Should Have a Carotid Stent?
Clinical
trial data continues to accumulate regarding the efficacy and safety of
carotid stenting. The current data indicates that the following
conditions favor carotid stenting with embolic protection over surgical
endarterectomy:
- High-risk patients where anesthesia and surgical repair would pose excess risk such as with congestive heart failure, uncontrolled angina pectoris, and severe obstructive pulmonary disease.
- Anatomic
characteristics that increase risk of carotid endarterectomy such as
previous radiation therapy to the neck, previous radial neck dissection,
restenosis after endarterectomy, and contralateral laryngeal palsy.
References
(1) Hunt JL, Fairman R, Mitchell ME et al. Bone formation in carotid plaques: a clinicopathological study. Stroke 2002 May; 33(5):1214-9.
(2) Roman
MJ, Naqvi TZ, Gardin JM, Gerhard-Herman M, Jaff M, Mohler E. Clinical
application of noninvasive vascular ultrasound in cardiovascular risk
stratification: a report from the American Society of Echocardiography
and the Society of Vascular Medicine and Biology. J Am Soc Echocardiogr 2006 August; 19(8):943-54.
(3) Prevention
of stroke by antihypertensive drug treatment in older persons with
isolated systolic hypertension. Final results of the Systolic
Hypertension in the Elderly Program (SHEP). SHEP Cooperative Research
Group. JAMA 1991 June 26;265(24):3255-64.
(4) Antiplatelet
Trialists' Collaboration. Collaborative overview of randomised trials
of antiplatelet therapy--I: Prevention of death, myocardial infarction,
and stroke by prolonged antiplatelet therapy in various categories of
patients. BMJ 1994 January 8;308:81-106.
(5) Mohler ER, III, Delanty N, Rader DJ, Raps EC. Statins and cerebrovascular disease: plaque attack to prevent brain attack. Vasc Med 1999;4(4):269-72.
(6) The
Stroke Prevention by Aggressive Reduction in Cholesterol Levels
(SPARCL) Investigators. High-Dose Atorvastatin after Stroke or Transient
Ischemic Attack. The New England Journal of Medicine 2006 August 10;355:549-59.
(7) Beneficial
effect of carotid endarterectomy in symptomatic patients with
high-grade carotid stenosis. North American Symptomatic Carotid
Endarterectomy Trial Collaborators. N Engl J Med 1991 August 15;325(7):445-53.
(8) Mohler ER, III. Carotid stenting for atherothrombosis. Heart 2007 September;93(9):1147-51.
(9) Endovascular
versus surgical treatment in patients with carotid stenosis in the
Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a
randomised trial. Lancet 2001 June 2;357(9270):1729-37.
(10) Yadav JS. Carotid stenting in high-risk patients: design and rationale of the SAPPHIRE trial. Cleve Clin J Med 2004 January;71 Suppl 1:S45-S46.
(11) Yadav JS, Wholey MH, Kuntz RE et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med 2004 October 7;351(15):1493-501.
(12) Sacco
RL, Adams R, Albers G et al. Guidelines for prevention of stroke in
patients with ischemic stroke or transient ischemic attack: a statement
for healthcare professionals from the American Heart
Association/American Stroke Association Council on Stroke: co-sponsored
by the Council on Cardiovascular Radiology and Intervention: the
American Academy of Neurology affirms the value of this guideline. Circ 2006 March 14;113(10):e409-e449.




