
Parasomnias are unwanted and uncontrolable events which happen during sleep.
They can be distinguished according to whether they occur during sleep onset, slow wave sleep or REM sleep.
- Those which occur in REM sleep are combined with affective disturbances and physiological stress reactions (fear, sweat, heart rate acceleration).
- The others (during slow wave sleep), on the other hand, leave the sleeper with very few memories.
Yet, this predisposal to have parasomnias or not is under the influence of all exterior factors which are able to act on the depth or architecture of sleep, this effect being described as "somnotoxic":
- Numerous somnotoxic "life events" (bereavement, moving houses, illness ...);
- Sport (competition, bedrest).
- Sleep deprivation and phase shifts (Cf " Night work" , "Jetlag" )
- Sleep pils can occure very serious parasomnias.
Their caretaking can usefully combine measures of sleep hygiene, behavioural cognitive therapies, and sometimes learning relaxing techniques. Very rare particular cases require the use of medications.
- SLEEPWALKING
This disorder occurs during slow deep sleep.
In the most spectacular cases, the person gets up and walks. More frequently, he/she sits up in bed and moves like if he/she was awake.
Nb. These gestures must not be confused with those, often more inconsistent and stereotypical, which occur during an attack of epileptic kind.
The sleepwalking subjects generally do not remember the episode after they have quietly gone back to sleep.
NB.Some scientists suggest to classify sleepwalking in the same category as other parasomnias* like nocturnal terrors or confusional arousals.
« A SLEEPWALKER SHOULD NOT BE WOKEN UP.»
Like for nocturnal terrors or confusional arousals, sleepwalking is a part of parasomnias, which can be seen like an inability to get out of sleep properly and completely.
It is therefore difficult to wake up the subject and he/she risks to show signs of confusion and irrational fear.
"The only risk you would take by waking up a sleepwalker is not to succeed or not to be able to explain him/her what he/she is doing outside of his/her bed and, if he/she has a bad character, he/she can get angry above all".

- Sleepwalking can lead to accidents
Sleepwalking is a disorder linked to the mutation of a gene very close to the areas involved in the immune system, like most of the other parasomnias.
According to Dr Mehdi Tafti, in Molecular Psychiatry, January 2003
«It is the same gene as for narcolepsy, but another allele. People who carry the allele have 3,5 times more risks to be sleepwalkers than others.
Currently, we know about 40 different alleles of that gene. All of them aren’t harmful, still many different (autoimmune) diseases are associated with them.
- BRUXISM
Bruxism is a harmless slow wave sleep parasomnia where the subject
shows repeated contractions of the jaw bones, thereby making a grinding
noise, unpleasant to the people around him/her.
Their exist mouth guards for the rare more serious cases which wear out the teeth abnormally.
Like all parasomnias, bruxism can coincide with periods of stress.
- SLEEPTALKING
It is a sort of "vocal sleepwalking", probably related with slow sleep dream phenomenons.
If someone wakes up the sleeper, he/she only reports very vague memories (to the opposite of what happens during the real dreams of REM sleep).
These events are more frequent in some families.
Generally, they do not have any pathological character.
- NIGHT TERRORS.
They express a dissociated arousal phenomenon during slow wave sleep,
a borderline form between sleepwalking and sleeptalking which is very
common between 3 and six years (mostly in boys, like for sleepwalking).
They raise a lot of questions and worries in parents but are totally benign and leave the sleeper with no memory.
The little one wakes up his parents with heart breaking screams of terror but gives no explanation (when one manages to wake him/her up, which is useless) and falls asleep again after a little while.
If that happens again, measures are advised to diminish the slow wave sleep pressure, like insisting on the nap, for example.
- BEDWETTING
Bedwetting is a slow wave sleep pathology which, in these subjects, reveals to be too deep to allow arousal during the night.
The subject cannot manage to wake up during the night to go empty his/her bladder like children of the same age do.
The genetic origin of the disorder, evidenced by the frequency of family cases, is confirmed by the recent advances of the human genome exploring.
In fact, the cases of adult bedwetting are exceptional because of the lightening of sleep observed after the post-puberty period.
That way, 10% of the bedwetting children recover spontaneously between 5 and 15 years.
"Time is the best medicine", the Chinese said : "it heals eight sick people out of ten".
Nb. It is difficult to distinguish what one does and what happens.
Clearly, any random "patamedicine" heals eight sick people out of ten very well and there is no reason why the "winners" should doubt the efficiency of what they have done. That bias leads, thus, to encourage all sorts of beliefs around the "magic treatment" of bedwetting.
- A too deep sleep
The psychanalytical therapies have not proven to be, as such, more validated than behavioural techniques (diary, pipi stop ...)
Some medications are efficient to limitate the filling of the bladder during sleep and they can help the child to solve some problems but (in this case like in many others), "time is the best medication".
One child out of ten will see his disorder disappear spontaneously between 6 and 16 years.
No "miracle" therapy (osteopathy, homeopathy, phytotherapy, fooltherapy...) has ever proven an efficiency superior to the the natural evolution of the illness which generally recovers before 16 or 18 years (in the "worst" case).
- ELPENOR’S SYNDROME
The Elpenor’s syndrome is also called confusional arousal.
It is a parasomnia which is characterized by a state of semi consciousness favoured by the brutal interruption of a very deep slow wave sleep phase.
The sleeper is awake enough to make elaborated tasks (like driving or fighting) but confusion affects his/her judgement and leads him/her to prejudicial behaviours.
The concept of Elpenor’s syndrome mainly responds to a juridic definition.
If there is no offense, it is is simply referred to as sleepwalking, of which the risk of trauma is well known.
NB. These states are related with "complex sleepwalking behaviours", which are mainly caused by medications, for instance, the "new sleeping pills" and "dopaminergics".
- KLEINE-LEVIN SYNDROME
This very rare but relatively disabling affection mostly concerns teenagers and young men.
It is emblematic of the sexual parasomnias which have received the name of "Sexsomnias".
It is characterized by the ocurrence of attacks of hypersomnia during a few days, combined with mood and behaviour disturbances.
The patient appears to be sleepy and slightly obsessed, starts to eat too much (hyperphagia) and to show signs of "hypersexuality" with behavioural disinhibition (e.g. public masturbation).
The disorder is associated to a mutation of the third allele of the same gene as the one involved in narcolepsy (Neurology décembre 2002).
Paralysis and sleep hallucinationsl;
REM sleep behaviour disorder (RBD);
"Sexsomnias";
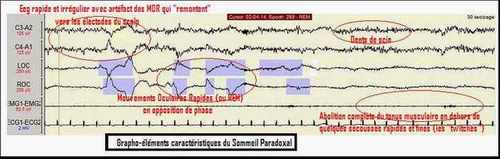
- REM sleep PSG
- DREAMING...
VOLTAIRE / Philosophical dictionnary
« Dreams have always been a great matter of superstition ; nothing was more natural. A man, deeply touched by his lover’s disease, dreams he sees her dying ; she dies the next day : so, the gods have foretold him about her death.
A general of an army dreams he wins a battle ; he wins indeed : the gods have told him he would be the winner.
We only take the fulfilled dreams into account and forget the others. »

- Nightmares : an intensely emotional content
Studies about the nature (chronology, imaginary part and primitive memory ...) and the meaning of dreams (premonition, after-life ...) have lead to large extend searches from Hippocrates to freudian psychiatry via the cold and slightly tendentious statistics of Soviet Union research.
None of these studies has finally been able to "interprete dreams".
Mentioning them sometimes brings the subject (or his/her psychotheapist) to interresting conclusions (and sometimes not...)
From our point of view, there is no reason to lose time in trying to find a meaning in dreams. At most, they can be considered like oddities which witness for a state of REM sleep.
Some individuals naturally dream more than others but it has no impact of any kind on the quality of their sleep.
NB However... While it would be useless to get lost in investigations about the meaning of the content of dreams, it is important to be able to recognize signs which witness for a psychiatric disease in their report.
A subject who suffers from depression, overwork (burnout) or from social phobia can have dreams with an evocative content for a specialist, which must be detected.
- SLEEP PARALYSIS
Check the article about "Paralysis and hallucinations during sleep", a frequent and harmless phenomenon at the root of many interpretative misunderstandings.
These phenomenons are particularly at the origin of a certain amount of "Sexsomnias".
Testimonies about "astral travel" and experiences of transcendental meditation of the tibetan munks and other kinds of levitations obtained in borderline states between sleep and wake and favoured by sleep deprivation, very frequent in adepts of ascetic life.
- Transcendental levitation or sleep hallucination

- REM sleep behaviour disorders (RBD)
Checl the article about "RBD".
It is a matter of differential diagnosis, sometimes difficult because of attacks of agitated sleepwalking (but they occur in slow wave sleep).
RBD matches an anomaly in the active abolition of muscle tone which normally occurs during REM sleep.
Therefore, the subject is able to move during his/her dreams.
That anomaly can lead to behaviours which are agressive against oneself or others, sometimes even with judicial consequences.
Their occurrence must lead to a neurological check-up in a sleep unit.
- SEXSOMNIAS.
"Sexsomnias" are involuntary behaviours with a sexual connotation.
"Sexual sleepwalkings" have been described, which express a slow wave sleep anomaly (dissociated arousal state)
REM sleep being associated with the appearance of an erection, some pathologies (dissociated dreaming) are complicated by enactment or interpreted like disorders with a sexual character.
- Incubus or succubus?
Their occurrence has been unnoticed for a long time because the subject is taboo but, thanks to the (courageous) action of sick people associations, it is now admitted that they can occur in 5 to 10% of the subjects treated with some medications like dopaminergics, used a lot in Parkinson’s disease and restless legs syndrome.