Acute Promyelocytic Leukemia
Author: Dr Frederick Appelbaum Fred Hutchinson Cancer Research Center Seattle 2008-07-28
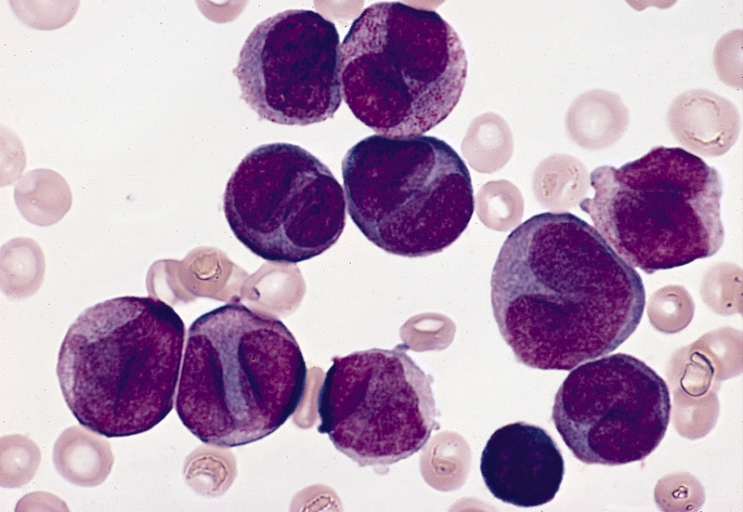
Acute Promyelocytic Leukemia (APL)
is a distinct subtype of AML
accounting for about 8% of cases. Patients with APL
tend to be younger on average than other AML
patients and are more often Hispanic. At the time of diagnosis, patients
virtually always present with some evidence of a coagulation disorder, with
easy bruising, petechiae or overt bleeding. A unique chromosomal
translocation, t(15;17), is found in virtually every case of APL.
Because of its unique clinical characteristics and response to specific agents,
APL is
treated differently from all other forms of leukemia.
Induction Therapy
APL is uniquely sensitive to two chemotherapeutic agents,
all-trans retinoic acid (ATRA) and arsenic trioxide. Clinical trials have
shown that induction chemotherapy that includes ATRA and an anthracycline
(daunomycin or idarubicin) is the preferred approach, and with these
combinations, complete response can be expected in approximately 90% of
patients. [7] Response rates tend to be higher in those patients
presenting with a white count less than 10,000/mm3. Occasionally
patients receiving ATRA will develop fever, shortness of breath and
abnormalities on chest X-ray. These can be manifestations of the so-called
retinoic acid syndrome, which usually responds quickly to treatment with
high-dose steroids.
Post Remission Therapy
Patients
with APL who achieve an initial
remission are treated with several cycles of consolidation chemotherapy,
usually using agents similar to those used during induction. Randomized
trials suggest that use of maintenance chemotherapy with ATRA alone or combined
with other agents for some period following consolidation (often up to a year)
is of further benefit. [8] With contemporary induction, consolidation and
maintenance regimens, approximately 60-70% of patients with APL are
cured. Because chemotherapy is so successful in APL, there is no
role for transplantation while patients are in first remission.
Recurrent Disease
Arsenic
trioxide is a very effective agent for the treatment of recurrent APL; approximately
80-90% of patients who relapse after initial therapy for APL will achieve a
second remission if treated with arsenic trioxide (assuming they have not
previously been treated with the drug). [9] Arsenic trioxide can cause cardiac
abnormalities and symptoms similar to those of the ATRA syndrome, and so should
be administered by individuals with experience in its use. Once patients
achieve a second remission, consideration should be given to pursuing an HCT.