2014/05/08

Tiredness is, here, often in the background. It results, according to the sick person, from the difficulty to face daily life with pains (of needle or burning sensation type) coming from any part of the body.
Recent studies tend to establish a parallel between fibromyalgia and chronic fatigue syndrome which could share a common physiopathological mechanism.
"Clinophilia" [2], that need to lie down in order to get some rest as often as possible, leads, sooner or later, to insomnia("wanting to sleep").
Statistics put forward an illness in which 80% of the sick persons are women, of late appearance, which would affect 2 to 3% of the population.
In our opinion, these numbers underestimate the existence of male or infantile forms of the disease that escape the actual recruitment criteria.
NB : "Fibromyalgia can evolve during years with a constant painful background punctuated with outbursts which often cause an important functional disturbance. Yet, according to the French Society of Rheumatology, its frequence decreases in a marked manner after 60 years to become exceptional after 70 years".
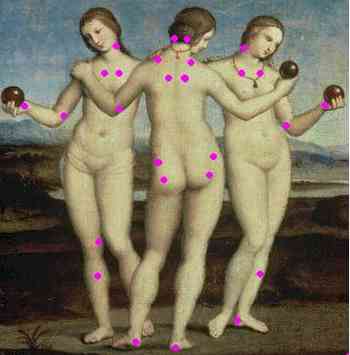
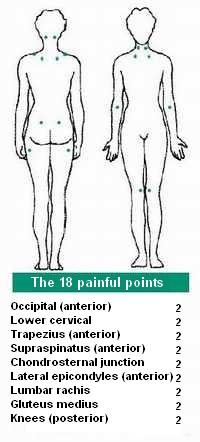
- Principal points that are abnormally painful at pressure
Definition
One of the best diagnosis criteria of the disease relies on the presence of a chronic and disabling painful chart at the root of a handicap that contrasts with the persistent absence of diagnosis after at least three different medical opinions over a period of at least three years. (This criteria eliminates, indeed, the majority of the potentially serious illnesses).
That chart is known by rheumatologists since 1904 under the tere of «muscular rheumatism». Despite the absence of modern means of exploration, they were forced to notice that that form of rheumatism did not evolve towards an aggravation with the loss of shape that characterize the other rheumatological diseases. (People said those were sick people who buried their doctor).
The first clinical descriptions of the "Idiopathic Diffuse Polyalgia Syndrome" (1970 : IDPS) stressed the existence of painful points in precise amount and places, which were singularly in contrast with the absence of medical explanations despite, often, very advanced check-ups.
With its cost and its occurrence in industrial societies, fibromyalgia has been the subject of very advanced studies but no official cause to it has been recognized.
We think that the role of sleep has been underestimated in actual research.
The hypothesis of the "hypo-sleep syndrome" stipulates that a disturbance of the sleep mechanisms can be at the root of these malfunctions of the systems of pain.
Fibromyalgia would appear at the stage of the "emergency stop" when the willpower of the subjet no longer manages to compensate tiredness.
Thus, it presents the four characteristics of the hypo-sleep syndromes : disabling, worrying, capricious and of good prognosis on the long term.
Still, it is impossible to deny the presence of an unefficient sleep and the difficulty of getting up in these sick people.
"The American college of rhumatology" defines, in 1990, Fibromyalgia with the existence of two «major criteria» combining diffuse pains and painful points retrieved during the clinical examination.
The pains are characteristic, of polyarthralgia type and muscle pains that rather occur in the morning, calmed by rest and aggravated during and after an effort).
The presence of anatomic points (tenderness points) that are abnormally sensitive to digital pressure (cf. illustration) sets the diagnosis in the absence of other disturbances. The criteria is accepted when at least 11 points out of 18 are retrieved.
That definition, maybe too strict, remains discussed.
Some doctors find up to 30 sensitive points, others stay «fibroskeptical» and doubt the reality of that entity (despite the recognition of the illness by the WHO) or make it a purely psychiatric pathology.
Recent publications attest, though, of an objective malfunction (FMRI) of cerebral zones implicated in the perception of pain in these sick people.
Clinical descriptions mention pain variations over time, according to climatic and hormonal changes, phyical activity, traumatic life events and overwork. They mainly concern the rachis area but can spread to the whole of the body.
Still, despite the ’absence of treatment and the sometimes very disabling side of the illness, the long term prognosis remains good and there is no incidence (other than iatrogenic) [3] ) on life expectancy.
The almost constant presence of associated symptoms described as « minor criteria » completes the chart in a very characteristic manner :
- They evoke, on one hand, the set of the socalled functional pathologies
The interview of the patient often reveals a very heavy medical or surgical past history (worth of being described as an assault course).
People mainly mention :- headaches, migraines, non specific ocular disorders (tiredness ...);
- colopathy, bloatedness, digestive pains, irritable bladder;
- atypical precordialgia, palpitations;
- dizzy spells, vaso-vagal faintness, pseudohypoglycemia or low blood pressure;
- swelling sensations, of joint stiffness, swarming or stinge sensations, sensations of electric discharges.
- some more seldom immune dysfunction syndromes (auto antibodies).
- a majority of patients are treated on the long course with thyroid extracts for functional insufficiencies of that gland, often made responsible (egg or chicken?).
- On the other hand, we observe the existence of disorders that
evoke a sleep disturbance like asthenia, weariness, nervosity and loss
of performance that can lead to an anxio-depressive chart out of
exhaustion.
Cognitive disorders are always present but they are in the background compared to pain (that difference is at the root of the very close chart of the chronic fatigue syndrome (cf.].
Three important details :
- The sleep disorders
are constant but insomnia, in itself, appears only very rarely amongst
the causes of consultation, to the point that doctors talked about a,
"insomniac who slept without difficulty".
We often notice, as a first step, a reaction voluntary hypersomnia. It all looks as though tiredness induced an attempt to "sleep more" which risks to end up, secondarily, in the vicious circle of insomnia - Most of the authors agree to distinguish fibromyalgia from a psychiatric disorder even if it shows narrow links with anxio-depressive syndromes (more frequent presence of familial or personal past history).
Even if it is frequent that some subjects present pathological personality traits, it may be rather a consequence than a cause of the illness and it is not the case of all sick people.
The anxious or anxio-depressive profile of the subject is no longer a sufficient criteria for the exclusion of the diagnosis of fibromyalgia.
- This sort of invisible, unexplained, disabling and discouraging diseases is, in itself, enough to cause authentic psychological disturbances.
- Tiredness, in its psychic and intellectual component, often shows pseudo-depressive sides : tears, loss of energy, loss of motivation, memory disorders.... which can be mistaken for signs of depression.
- Since clinophilia causes a phase advance (with a
too early bedtime), the awakening in the morning will occur too early
as well. Such a chart of morning insomnia in a tired subject can also be
looked at as a form of depression.
In our opinion, like in chronic fatigue or "spasmophilia", the
psychiatric diagnosis (depressive or anxious disorders) is widely
overestimated.
The fibromyalgia sick person is often confronted to a medical world that doesn’t always recognize the reality of the disease.
We think that fibromyalgia is not a simply psychosomatic pathology and that that a "psy" approach only leads to a loss of mutual trust between the doctor who "psychiatrizes" while the patient "somatizes".
That failure of the doctor-patient relationship is characteristic of the set of symptoms of hypo-sleep.
Here, it becomes so important that the term of "medical browsing" has been used to describe the defect of these "bad sick people" who change doctors all the time.
For the first specialists of fibromyalgia (F. Khan, 1981), the fact that several doctors (more than three or four) have been held in check is, in iself, a major diagnosis criteria.
- According to some studies, fibromyalgia may be more frequently encountered in women over 40 years
but the inclusion criteria are probably at the origin of a certain bias
since more recent studies mention fibromyalgia in men but also in
children.
In our opinion, the particular somnological ground is equally distributed between the genders and it is the events of life and the unequality of burdens and obligations which are at the root of this apparent disparity.
Physiopathological mechanism :
Since 1975, characteristic abnormalities have been shown in fibromyalgia patients. There exists, in the sleep architecture of these sick people, signs of hyperarousal, little specific but constant enough to make the disease to be recognized in 1990 in the international classification of sleep disorders (ICSD American Sleep Disorder Association) under the term of «fibrositis syndrome».
A disturbance of the slow deep sleep would be the first cause of a lowering of the pain perception point, a true hyperesthesis to external and internal stimulations of the organism. The sleep of the sick persons is unstable and we observe, in polysomnography, (Cf. sleep exploration) the abnormal presence of arousal signals (K-complexes) and burst of waves of wake stage (Alpha) during slow wave sleep (Delta). That type of sleep is called «alpha-delta sleep».
There may exist a dysfonction of the descending neurological inhibitor system in charge to block out the «background noise» of the organism. The present studies are about the presence of pain mediating polypeptides in excess in the brain of the sick person.
Etiopathogenic hypothesis
Fibromyalgia often presents a progressive mode of onset with numerous past episodes of multiple and varied functional disorders sometimes going back to childhood (repeated consultations and check-ups) but the chart sometimes gets worse after a more significant episode.
The triggering role of an infectious trauma has been mentioned. In fact the predisposing ground to the illness probably rather corresponds to a latent conflict between tiredness (due to a bad sleep efficiency of genetic origin and very often familial) and the strength of resistance written in the sick person’s personality itself.
According to our hypothesis, the efficiency of sleep is genetically unequal between the individuals. The sleep of the fibromyalgia patients may be very senstitive to life events.
In fibromyalgia , the psychological resistance mechanisms are shown by an excess of nervous tension which contributes even more to deteriorate the quality of sleep. The symptoms of fibromyalgia appear at the stage of decompensation of the vicious circle : when the subject’s reserves are exhausted.
We think that the attack of «spasmophilia (or tetany)» is a form of acute decompensation of the hypo-sleep syndrome.
With their early occurrence in the life of somebody, these attacks are signs that presage fibromyalgia. Their detection and their understanding could take part in a true prevention approach.
Treatment :
The «treatment» of fibromyalgia is difficult and some specialists more willingly speak about "taking care". The whole of the publications insist on the quality of the trust-relation between doctor and patient.
It is very important to try to define well fibromyalgia with the sick person. That allows, first, to limit the complementary explorations and the risk of iatrogenic accidents (= complications due to medical gestures). The sick person is relieved to know that it is a known illness, silent for a long time, and sometimes very disabling but with a good prognosis on the long term.
It is necessary to tell the person that there is, so far, no miracle treatment...
From our point of view, fibromyalgia is one of the stages of the "emergency stop" of the hypo-sleep syndrome.
It is the result of a long struggle against tiredness where the subject sinks into a true vicious circle (the train of the hypo-sleep syndrome).
Decompensation is the sign of defeat.

- A sometimes major functional handicap
From a therapeutic point of view, il is essentiel to motivate the sick person to do everything to reinforce the quality of his/her wake state :
- It is important, in the first place, to avoid all the factors that
can be harmful for sleep : alcohol, coffee, tranquillizers,
antidepressants....but also the many other medications often prescribed
without considering their "anti-sleep" effect.
- A very ponctual use (one or two evenings a week) of "sleep regulators" can contribute to "pay the debts, one by one" before the appearance of other signs of decompensation (cf. hypo-sleep syndrome). Thus, some sleeping pills of the new generation can be used as "sleep tonics".
- Many specialists of fibromyalgia advocate for the tricyclic
antidepressants like amitriptyline which is the reference long course
treatment of the evolved forms (its efficiency is not constant). The
present studies are about the selective serotonin reuptake inhibitors
(which would have the effect of reinforcing the quality of sleep).
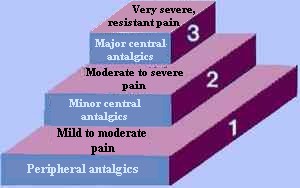
Other molecules are the subject of research (gabapentin, pregabalin, gamma-OH) but the results are discording. - The «symptomatic» treatments: first level antalgics (paracetamol) and anti-inflammatories are sometimes useful.
The second level antalgics are often of an inefficiency that is so characteristic that it enters, according to some, into the diagnosis criteria of the disease. On the other hand, numerous therapeutic habits "advocated in case of..." are disappointing in the long term . Their list is long but we must, here, point at the magnesium, calcium and the oligo-éléments, that the majority of the sick people have been brought to "try" despite the «absence of specifically demonstrated therapeutic activity».
- Numerous illusory treatments (issued from the "pseudosciences")
often get the support of a large number of sick people for a while but
none of the many alternative therapies offered on the market has, so
far, proven its efficiency.
The individual results observed hither and tither are probably caused by a change of life hygiene and by the therapeutic effect coming from the trust relation between the therapist and the sick person.
That effect unfortunately never lasts and the loss of efficiency could harm that doctor-patient relationship.
Beware of the miracle drugs offered on the lucrative market of tiredness or of fibromyalgia. It is an evidence that if they kept their promises, fibromyalgia would not be what it is...
The directions of research in 2007 ...
The new class of medications of the endocannabinoid system could reveal to be promising.That system of complex neuromediators of recent discovery appears to be the common orchestra conductor to the mechanisms of pain (in the heart of fibromyalgia), immunity (herpes, allergies), appetite (obesity, thinness), mood (anxiety, tears, "depression") and sleep regulation (slow wave and REM sleep power).
It is striking to notice the correlation between those systems and the problematic of the fibromyalgia patients.
A molecule that should arrive soon on the French market with the indication of "depression and sleep disorders", seems, to our mind, to be theoretically promising with acting directly on the melatonin brain receptors. That process comes from the fact that oral melatonin revealed unefficient because it doesn’t reach the brain.
To be continued ...
The «caretaking»
Whether there exists, or not, a medication treatment, it seems fundamental to us to consider fibromyalgia like a chronobiological sleep pathology.
The notions of sleep hygiene are in the center of a global therapeutic approach.
"To sleep well, one must have been awake well" (Zarathustra said).
The mechanisms of the wake/sleep alternation and notions of structure and quality of sleep must be explained to the patient.
Make him/her understand that sleep is initiated by the activation of permissive networks by hormones that are synthesized during wake state, that, far beyond the ease to sleep "like a baby", the quality of sleep itself depends from the quality of the previous wake state.
Just like for the care of obesity (where a food diary must be kept), it is important to be able to proceed to an analysis of the somnological characteristics of the patient (short/long sleeper ?, owl/lark? flexible or rigid?) with the help of tests and of the analysis of an sleep/wake diary..
These information are important for the implementation of techniques designed to reinforce sleep efficiency.
- 1. Managing the nap, its indications and contraindications must be strictly adapted to the somnological profile of the person ("Sleep is individual and deserves individual information").
- 2. (Moderate) physical activity and sunlight have an
awakening "amphetamine-like" effect. For that reason, these two factors
are indispensable for the quality of sleep.
Physical activity must be particularly soft and progressive. It tends to a re-appropriation of the physical abilities with a very gradual training. Experiments of gymnastics in groups in a warm swimming pool are said to be organized by the CHU of Lille, with good results.
Physiotherapy in warm water (swimming pool or spa) seems to give promising results.
Phototherapy with "day like" bulbs and «thermotherapy» (sport, hammam ...) take part in the indispensable change of life for the care of the fibromyalgia patient (like in all the other functional disorders).
Some methods of manual therapies are indispensable complements for the implementation of a program for the readaptation of the organism to the effort. Physiotherapy, spa bath therapy, thermalism, relaxation methods and, sometimes, psychotherapy, can contribute to reactivate the wake circuits.
The cognitive and behavioral treatments have prooved efficient when demoralisation, inactivity, pessimistic thoughts and boredom play a key role in the maintaining of somatic pains (sometimes in conjunction with personality disorders).
Phototherapy lamps might be very interesting in fibromyalgia patients (the point is to expose retina to an electric light intensity strong enough to influence the internal biological clock through melatonin).
It is to be deplored that those relatively inexpensive equipement are not taken in charge by the National Health Service.
Sleep better, sleep little, live better...
All in all, recovery depends mainly on the participation of the sick person. He/she will have to modify his/her sleep and life hygiene habits.
All the difficulty consists in gathering the conditions of a restful sleep in a society that leaves little choice. The modern rythms of life and work are often similar to a double or even triple day... (Active women are, for that reason, particularly victims of an important overwork and there is probably, there, a cause of the prevalence of the disease in women.).
Fibromyalgia never heals easily. It must be managed on the long course. The patient, implicated in his/her own caretaking, can recover an optimal functional status as long as he/she has learned not to exceed his/her limits concerning his/her sleep.
Moreover, just like a former obese keeps the result of his/her diet if he/she continues to control his energetic intakes and expenses, the "ex" fibromyalgia patient must be able to maintain a necessary and sufficient level of physical activity ; the "SMIG" (Minimum of Sport Indispensable to People).
Tiredness or sleepiness ?...The misunderstanding at the heart of the problem.
Never mix up ! :
—Sleep insufficiency shows through sleepiness and the nap can then be an emergency somnication.
—An excess of sleep aggravates tiredness and fibromyalgia is thus a logical contraindication to the nap.
Nb. A bit of "ethno-fibromyalgia" ?
In Guadeloupe, there is an illness, well known by the population of the remote regions of the coast under the wind, that remains mysterious for the medical profession.
It is the "BLESSE" (blessure=wound) that strikes the victims of a trauma, sometimes seemingly harmless (flu, an accident, an argument...) but which is the starting point of a syndrome that is very close to fibromyalgia.
"Doctor, my whole body hurts and I have a "gas" that goes up to my head and down to my stomach.. And I feel weary, even if, if, if, if !"
Like for fibromyalgia or chronic fatigue, the hospital check-ups are of no use in that chart that is not a "bitin pour docteur" and people must turn to the wizard (Kimboiseur) to try to heal that "maladie à Bon Dieu" with massages and "kimbois" (magic) of the "frotteur de blesse" ...
Generally, that "treatment" is quite painful and the "kimbois" are often expensive but "one has to" "kimmbé raid" (stand fast).
Kimmbé Raid moun Guadloup, ni un jouw ça ka finiw !!
Footnotes
[1] A symptom or set of symptoms is described as "functional" when it is not caused by a lesion that can be identified
[2] This term describes the constant need of lying down to get rest every time it is possible.
[3] The
adjective iatrogenic is used to describe « every undesirable
consequence on health of any medical act aiming to preserve it"