2008-07-28
Abdominoplasty ( tummy tuck ). What it is, who it's for, techniques, results and risks.
Abdominoplasty is technique for surgically removing excess fat and skin from the abdominal wall, and in some cases repairing weak or separated muscles, to produce an abdominal profile that is smoother and firmer. It is most effective in persons of normal weight who have loose, sagging skin. The excess skin is removed, and a permanent improvement in contour is accomplished. This Knol explains what it takes to achieve good results, describes the techniques available, lists the possible complications, and suggests the steps someone considering this surgery should take.
Introduction
Even with diet and exercise, a tight smooth abdomen may not be possible if the skin is stretched and sagging, if the supporting tissue is weak, or if there are scars from previous surgery producing irregularities. The most common causes of flaccid, stretched skin are heredity, multiple pregnancies, fluctuations in weight, and significant weight loss. Exercise will tone the abdominal wall musculature but it will not tighten saggy skin. Liposuction can remove fat deposits under the skin but does not correct sagging, and actually could worsen the appearance of flaccidity by removing the fat that underlies and supports the skin. No externally applied creams, substances, or devices are effective for tightening significantly stretched skin. By removing the excess skin surgically, abdominoplasty improves the external appearance of the abdominal wall and restores the smooth, slim contour of the youthful body.
Abdominoplasty is not a substitute for weight loss, and is not useful in obese individuals. The
operation is designed to remove loose skin. A thick fat layer under the
skin causes protrusion and these thick rolls of fat not only limit the
ability to remove excess skin but also interfere with safe wound
closure. In addition, abdominoplasty should not be done in
individuals who are planning to lose weight. A surgical improvement in
the contour of the abdomen will be reversed if the person subsequently
loses a substantial amount of weight and the skin again becomes loose
and hanging.
The
surgery is best performed on adults of any age who are in good health,
close to the ideal weight for their body type and size, and are
moderately fit with good muscle tone.

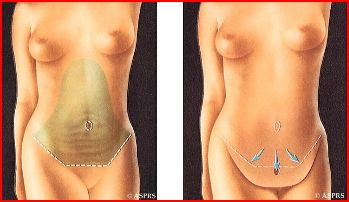
The photographs in this post are from the website for the American Society of Plastic Surgeons and more can be seen at www.plasticsurgery.org
Statistics from the American Society of Plastic Surgeons about
abdominoplasty give a picture of patients who elect to have this
surgery:
· 5th most common cosmetic surgery performed by Board-certified plastic surgeons
· 148,410 patients in the United States had an abdominoplasty in 2007
42% were age 40-54
34% were age 30-39
13% were age 55 and over
10% were age 20-29
None were under the age of 20
· 96% of the patients are women
Basic considerations about abdominoplasty
Planning for an abdominoplasty involves sorting out a number of elements that contribute to the overall picture of a loose, sagging abdominal wall. These vary in expression but are the factors that determine which of several surgical approaches will be most effective in any given individual. These include:
· the degree of skin redundancy and flaccidity
· the location of the skin laxity with regard to landmarks like the navel, called the umbilicus, and the crease above the pubic bone
· the amount of fat under the skin and its location, especially if it is localized
· separation of the abdominal wall muscles which is called diastasis recti
· laxity of the fibrous layer of the abdominal wall which is called the musculoaponeurotic fascia
· the presence and location of scars and stretch marks which are called striae
Plastic surgeons classify abdominal wall deformity based on the severity of these basic features (1)
and then use the classification system to select the most appropriate
surgical technique according to the severity of the composite picture. (2) For
example, moderate skin excess with no diastasis could be treated with a
miniabdominoplasty (description below) while significant skin excess
with fascial weakness would be addressed with a traditional
abdominoplasty and diastasis repair.
Scars and striae (stretch marks)
Pre-existing
scars deserve attention because they represent areas where the skin was
previously undermined or elevated, which disrupts blood supply. The
skin around the scars may not have enough vascularity to survive
additional surgical mobilization which means that skin loss or serious
wound healing problems can occur with further surgery. If the scars are
situated where they can be removed at the time of abdominoplasty, as is
usually the case with Caesarian section scars, the problem is solved. However, large scars on the upper abdomen are a contraindication to proceeding with abdominoplasty in some cases. In one series, the rate of complications was three times higher in patients with scars on the upper abdomen. (3)
Some
striae, or stretch marks, are removed at the time of abdominoplasty if
they are located on the excess skin that will be removed. Those
distant from the surgery will remain, but the appearance of these
striae generally is improved greatly by the overall skin tightening
accomplished with abdominoplasty.
Gender differences
Patterns
of fat distribution vary with sex, age, and heredity. Women have a
higher percentage of total body fat than men and typically accumulate
fat in the lower abdomen, around and below the umbilicus, in what is
called a gynoid pattern. The distribution in men is more generalized, involving the entire abdomen and torso in an android pattern.
Because of this and other gender specific differences, there are
technical differences between the male and female abdominoplasty. Some of these include:
- Men have thicker skin than women and may do well with liposuction where a woman would see accentuation of skin laxity and sagging
- Except in cases of massive weight loss, the amount of skin removed with abdominoplasty is less extensive in men than in women
- The upper border of the pubic hairline is less defined in a man than in a woman so the skin incision generally is placed in a location different from that in a woman
- Many men with a prominent abdomen have a great deal of intra-abdominal fat which is not addressed by either abdominoplasty or liposuction of the abdominal wall
Various techniques used for abdominoplasty
There are several technical variations with abdominoplasty, largely because the complex composite of basic problems to be corrected vary from patient to patient. These are reviewed below but it is helpful to recognize that they are variations of a series of basic surgical steps that are part of any abdominoplasty. These basic steps include:
- a horizontal skin incision low on the abdominal wall between the umbilicus (navel) and the pubic hairline
- separation of the abdominal skin and fat layer from the underlying fascia covering the muscles
- a circular incision around the umbilicus leaving it in place, attached to the underlying fascia as an isolated island
- separation or elevation of the flap of skin and fat layer up to the level of the ribs above if needed
- repair of weakened abdominal muscle fascia if needed
- drawing the flap of skin and fat toward the feet until it is taut, removing the excess overlapping skin and fat, and securing the tissue in place
- creating a new opening in the flap that has been drawn tight, through which the umbilicus can be brought out again and sutured in place
Skin incisions

The
principle with the skin incision is to place it where the resultant
scar will be concealed as well as possible within naturally occurring
skin creases and will be covered by underwear and swimwear. This
usually means placing it at the level of the pubic hairline in women
and somewhat higher in men. The shape and length of the incision and
scar are determined by the degree of correction necessary. When the
surgery will be isolated to the area below the navel, a shorter incision
can be used. If there is overhanging skin extending towards the hips at the sides of the abdomen, a longer incision is needed.
Musculofascial repair
 Repair
of the fascia, the fibrous layer covering the surface of the muscles,
is indicated in patients where this is lax. In general, this involves
folding or overlapping the loose tissue and suturing it together in the
tightened position. One of the most common forms of fascial laxity is diastasis recti where the fascia running vertically between the rectus muscles is stretched out. Often
seen after pregnancies, this laxity is corrected by sewing the fascia
over the two rectus muscles back together in the midline.Umbilicus (navel)
Repair
of the fascia, the fibrous layer covering the surface of the muscles,
is indicated in patients where this is lax. In general, this involves
folding or overlapping the loose tissue and suturing it together in the
tightened position. One of the most common forms of fascial laxity is diastasis recti where the fascia running vertically between the rectus muscles is stretched out. Often
seen after pregnancies, this laxity is corrected by sewing the fascia
over the two rectus muscles back together in the midline.Umbilicus (navel)
When
moving the skin and soft tissue on the abdominal wall, the umbilicus
presents a challenge since it needs to remain located in the midline at
the level of the top of the hipbones when the abdominoplasty is
completed. As a consequence, it is cut free and left in
place as a small island while the skin flaps are moved and secured. An
incision is then made to serve as a new opening through which the
umbilicus on its island stalk is brought out and sutured to the skin. This results in a circular scar around the umbilicus. For
an abdominoplasty where the surgery will be isolated to the area below
the navel, this work with the umbilicus may not be necessary.
It order to preserve blood supply and maintain the viability of the skin flaps elevated and moved during abdominoplasty, liposuction is not done in the same surgical area. However, it can be used at the margins of the abdominoplasty surgery. For example, it often is used in large abdominoplasties to tailor areas along the sides of the body, such as the flanks.
Specific techniques
The traditional abdominoplasty described above has several variations that enjoy separate names, including:
- Mini-abdominoplasty. (5) This is a limited abdominoplasty, useful when the excess skin and fat are primarily below the umbilicus and is suitable for individuals whose problems are too slight to require a standard abdominoplasty. With the mini-abdominoplasty there is a shorter upturned incision and the position of the umbilicus does not need to be adjusted.
- Fleur-de-lis abdominoplasty. The name refers to an inverted T- type of abdominoplasty which is useful for individuals with large amounts of excess skin, such as those who have lost massive amounts of weight. The “T” portion of the surgery on the upper abdomen permits adding side-to-side tightening of the abdominal wall.
- Belt lipectomy. (6) This technique involves an abdominoplasty on the anterior abdomen but continues incisions to encircle the torso in order to remove excess skin and fat over the sides, buttocks and back. Most commonly, it is used for individuals who have undergone massive weight loss.
- Umbilical float. This technique may be used in conjunction with a mini-abdominoplasty to avoid the incision and scarring around the umbilicus. Here, the umbilicus is left attached to the skin, cut loose from the underlying abdominal fascia, and allowed to descend or “float” toward the pubic area as the skin is tightened. This shortens the distance between the umbilicus and the pubic bone so it is not suitable if the distance will be shortened greatly.
Complications with abdominoplasty
Data collected from a number of studies show that complications are common, occurring in 12-32% of abdominoplasty cases. (7) The more common complications of abdominoplasty are wound infection, blood collection in the treated area (hematoma), fluid collection in the treated area (seroma), skin loss along the edges of the incision, and minor wound separation. More major complications are reported in 1.4% of cases and these include major skin loss, deep vein thrombosis, and pulmonary embolus.
Patient
factors that correlate with a higher incidence of complications are the
presence of diabetes, hypertension (high blood pressure), and smoking.
Complications are magnified dramatically in obese patients with one
series reporting complications in 86% of obese patients and another
reporting them in 80% of obese patients. (8)
Who are candidates for abdominoplasty?
Abdominoplasty addresses loose, sagging skin and soft tissue on the abdominal wall. In addition to skin laxity, factors to consider include:
- General health. Persons with significant medical problems such as severe cardiac or lung disease and those with pre-existing health conditions that impair wound healing or diminish the ability to combat infection should not have an abdominoplasty.
- Body weight. An abdominoplasty is not a treatment for obesity and the ideal patient is at or near his or her ideal body weight. Adherence to this guideline results in fewer serious complications and in higher patient satisfaction after the surgery because the results are better. As mentioned above, the surgery should be postponed in individuals who are planning substantial weight loss.
- Future pregnancies. For women who are planning future pregnancies, an abdominoplasty should be postponed until after child-bearing. This minimizes any impact of surgical after-effects on the pregnancy and delivery. It also avoids reversing the surgical improvement in the contour of the abdomen that would occur if the person again went through a pregnancy with recurrence of skin laxity.
- Age. Age itself is less important than general good health and appropriate body weight.
- Type of anesthesia required. For a miniabdominoplasty, surgery can be done with local anesthesia and sedation in an out-patient setting. For a traditional abdominoplasty with diastasis repair, deeper anesthesia is needed and this should be administered in an accredited surgical facility with appropriate monitoring equipment, the ability to give fluid resuscitation, and postoperative monitoring capabilities.
- Medications. Patients who are taking anticoagulants or blood thinners should not have an abdominoplasty due to the bleeding risk. Other medications, including vitamins, herbal supplements, and over-the-counter drugs need to be reviewed before surgery and some may need to be discontinued. Aspirin and anti-inflammatory drugs can increase bleeding; medications for a variety of diseases, such as rheumatoid arthritis, can impair wound healing.
- Smoking. Nicotine in cigarette smoke causes constriction of the blood vessels in the treated tissue which can result in diminished blood supply, or ischemia, and loss of the overlying skin. Smoking cessation is required well in advance of the surgery.
- Expectations. Individuals interested in an abdominoplasty should consider why they want the surgery and their expectations about the outcome. In dialogue with the surgeon, informed consent should flow from a full understanding of the surgical technique, alternatives, risks, and potential complications.
- Recovery time. Drains are used to collect any fluid that accumulates under the abdominal skin after surgery. These drains generally are removed a week or two after the surgery. In addition, an elastric abdominal binder, or girdle, is used after an abdominoplasty to prevent the accumulation of fluid, limit swelling, and smooth the contour of the treated area. Depending on the magnitude and location of the surgery, the time away from work and from physical exercise may be up to four weeks.
- Costs. The price of abdominoplasty is variable depending on where it is done, the type of anesthesia, and the amount of surgery done with the technique selected for the individual. Statistics from the American Society of Plastic Surgeons show the average physician fee in 2007 for an abdominoplasty was $5,264. An abdominoplasty is cosmetic surgery and the costs are not covered by health insurance when it is being done for elective body contouring. When the technique is used as part of the treatment for a medical disorder such as skin breakdown due to extreme redundancy after massive weight loss, health insurance may provide coverage benefits.
Steps potential patients should take
When
an individual is considering a surgical procedure like an
abdominoplasty a thorough consultation with a plastic surgeon is the
first step. Because there are so many techniques based on individual
variations in the presenting problem, a comprehensive examination and
discussion are needed before settling on the right operation for any
individual. It is important for a plastic surgeon to have
familiarity with a variety of techniques and applications, and the
availability of trusted anesthesiologists and staff is essential.
One
way of finding a competent, skillful and communicative plastic surgeon
doctor is to look in the ranks of trained, Board-certified surgeons,
credentialed at an accredited medical facility. Resources
are available to help with this, and the following Web sites can provide
further information and the names of surgeons who have met professional
criteria, including requirements for ongoing medical education and
interval reexamination for maintenance of certification.
Plastic surgeon referral service 1-888-4-PLASTIC (1-888-475-2784)
American Society of Aesthetic Plastic Surgery
(3) Cardoso de Castro C et al: How to deal with an abdominoplasty in an abdomen with a scar. Aesthetic Plast Surg 17:67, 1993.
(4) Matarasso A: Liposuction as an adjunct to a full abdominoplasty. Plast Reconstr Surg 106:1197, 2000.
(5) Greminger RF: The mini-abdominoplasty. Plast Reconstr Surg 79:356, 1987.
(6)Aly AS, Cram AE, Chao M, etal: Belt lipectomy for circumferential truncal excess: the University of Iowa experience. Plast Reconstr Surg 111:398, 2003.
(7) Hensel JM, Lehman JA Jr, Tantri MP, et al: An outcomes analysis and satisfaction survey of 199 consecutive abdominoplasties. Ann Plast Surg 46:357, 2001.
(8) Vastine VL, Morgan RF, Williams GS, et al: Wound complications of abdominoplasty in obese patients. Ann Plast Surg 42:34, 1999.
(4) Matarasso A: Liposuction as an adjunct to a full abdominoplasty. Plast Reconstr Surg 106:1197, 2000.
(5) Greminger RF: The mini-abdominoplasty. Plast Reconstr Surg 79:356, 1987.
(6)Aly AS, Cram AE, Chao M, etal: Belt lipectomy for circumferential truncal excess: the University of Iowa experience. Plast Reconstr Surg 111:398, 2003.
(7) Hensel JM, Lehman JA Jr, Tantri MP, et al: An outcomes analysis and satisfaction survey of 199 consecutive abdominoplasties. Ann Plast Surg 46:357, 2001.
(8) Vastine VL, Morgan RF, Williams GS, et al: Wound complications of abdominoplasty in obese patients. Ann Plast Surg 42:34, 1999.