Author: Dr Paul W. Ladenson Johns Hopkins University 2008-06-10

Thyroid cancers are
malignant tumors in the thyroid gland, a butterfly-shaped organ draped
around the front and sides of the windpipe (or trachea) in the lower
neck. (Figure 1) There are several types of thyroid cancer, each with
its own characteristics (Table 1); papillary thyroid cancer is by
far the most common. Thyroid cancer occurs in women three times more
often than men.
The incidence of thyroid cancer rises with age, and the
types that occur in older people are generally more aggressive. However, certain forms of thyroid cancer (e.g., papillary and medullary cancers) can also appear in childhood and adolescence.Figure 1. The appearance and anatomic relationships of a normal thyroid gland

Thyroid
cancers vary widely in their seriousness and the intensity with which
they must be treated. Some tumors are tiny—only detected at surgery or
imaging for another reason—and probably would never have affected a
person’s health. Even individuals whose thyroid cancer is found as a
thyroid lump (nodule) are usually cured by surgery and other
minimally disruptive treatments. But when thyroid cancer has spread
outside of the neck, or when thyroid cancer is an aggressive subtype,
the disease can be difficult or even impossible to treat. Thyroid
cancers that are widespread and have lost the characteristics of normal
thyroid cells, so called poorly differentiated cancers, can be life-threatening.
Treatment
of most thyroid cancers begins with surgical removal of the thyroid
gland. Then radioactive iodine, which is taken up by normal thyroid
cells and many cancers, is used in selected patients to eradicate
residual disease. After their initial treatment, people with treated
thyroid cancer must take thyroid hormone medication daily to replace the
function of their missing gland, and prevent any potentially remaining
thyroid cancer tissue from growing back. Because thyroid cancer often
comes back after being apparently effectively cured, people who have
been treated for thyroid cancer must be monitored—usually for the rest
of their lives—to detect and treat any residual disease at an early
stage. Treatments for thyroid cancers that cannot be removed surgically
or killed with radioactive iodine may include external beam radiotherapy
and/or chemotherapy What Does the Thyroid Gland Normally Do?
The thyroid gland’s follicular cells make and release into blood two small chemicals, called thyroid hormones, thyroxine (T4) and triiodothyronine (T3). Each of them is comprised of a pair of amino acids to which iodine molecules are attached. The iodine needed for thyroid hormone production comes from our diet. Once absorbed, iodine in blood is trapped by a special pump in thyroid cells, called the sodium-iodide symporter. Thyroid follicular cells also have several specialized biochemical ‘fastening machines,’ called enzymes, that then carry out the steps needed to attach iodine to particular parts of a very big protein called thyroglobulin, which is made only by thyroid cells. These special molecules present in follicular cells of the thyroid, the sodium-iodide symporter and thyroglobulin, are important in evaluating patients with so called differentiated thyroid cancers (i.e., papillary, follicular, and Hürthle cells cancers), as described below.
In
the nucleus of almost every cell, thyroid hormones bind to molecules
called T3 receptors, which are attached to segments of DNA that regulate
certain genes. Precise control of how many proteins are made from these
genetic blueprints maintains the normal, or euthyroid, thyroid state.
Whether the thyroid hormone come naturally from the thyroid gland itself
or from thyroid hormone medication, excessive activation of these genes
by abnormally high thyroid hormone levels cause hyperthyroidism;
whereas, inadequate gene activation due to insufficient thyroid hormone
production, such as after thyroid surgery, causes hypothyroidism. (See
Knols on Hyperthyroidism and Hypothyroidism.) The thyroid normally makes
precisely the right amount of its hormones under the exacting control
of the pituitary gland, which is an extension of the brain. Specialized
pituitary cells make thyroid stimulating hormone (TSH), which travels in
blood to the thyroid gland, where TSH binds to its own receptors on
thyroid cells, prompting them to grow and produce more of the thyroid
hormones. Normally, this system is kept in balance by the negative
feedback of the thyroid hormones on TSH-secreting pituitary cells (as
well as the part of the brain that controls them).
For people
with thyroid cancer who have had their thyroid gland removed surgically,
thyroid hormone medication (levothyroxine [L-thyroxine]) must be given
to replace the function of the gland. In differentiated thyroid cancer
patients, thyroid hormone treatment is also important to suppress the
pituitary’s production of TSH, which could promote regrowth of thyroid
cancer tissue.
The thyroid gland also contains another population
of cells, called parafollicular or C cells, which produce another
hormone called calcitonin. Although calcitonin appears to have no
essential function in humans, it can be useful to identify people with a
malignant C cell thyroid tumor, called medullary thyroid cancer.
Furthermore, high blood levels of calcitonin in patients with
widespread medullary thyroid cancer can cause symptoms of diarrhea,
flushing, or itching, as described below.
How Common is Thyroid Cancer?
In 2008, there will be more than 37,000 new cases of thyroid cancer in the United Stated, and 1,590 Americans with thyroid cancer will die of their disease. Because thyroid cancers are usually effectively treated, it is estimated that there are more than 300,000 survivors of thyroid cancer in the U.S. Thyroid cancer is more common in women, older persons, and whites. Women whose pregnancies are later in life and obese people have also been found at greater risk of developing thyroid cancer. Thyroid cancer is becoming diagnosed more commonly in the U.S., and currently has the fastest rising incidence of any malignancy in U.S. women and in older persons. (Figure 2) This is due, in large part, to detection of small thyroid cancers that previously went undetected.
What Causes Thyroid Cancer?
Scientists are learning how derangements in certain parts of the DNA genetic blueprint that controls thyroid cells’ growth can lead to thyroid cancer. For most people with the condition, however, a specific underlying cause of their thyroid cancer remains unknown. Certain genetic and environmental factors that increase risk of developing thyroid cancer have been identified. Some types of thyroid cancer are inherited or familial. In one-half of people with medullary thyroid cancer, for example, there is an inherited mutation in a specific part of their genetic blueprint, the Ret gene, that makes it almost inevitable they will develop thyroid cancer, often early in their lives. Genetic testing can be performed to predict which children and other relatives are at risk of acquiring the condition. Papillary thyroid cancer, a more common type of thyroid malignancy, also affects a close family member in about one in ten cases; but the genetic mutation(s) responsible for familial papillary thyroid cancer has not yet been discovered, so testing currently doesn’t exist to predict which relatives are at risk.
Radiation of the thyroid gland,
especially in childhood and adolescence, can predispose to later
development of thyroid cancer. Two kinds of radiation exposure have been
implicated. First, x-rays were used to treat a number of minor diseases
in children between the 1920s and early 1950s, mainly in the U.S. These
conditions included inflammation of the tonsils and adenoids, acne,
ringworm, and some kinds of birthmarks. As many as one-third of these
previously irradiated children—now people in their sixties and
older—will be found to have a thyroid cancer with careful investigation.
Second, radioactive iodine released after nuclear reactor accidents or
fallout from atmospheric nuclear weapon testing or use predisposes to
development of thyroid cancer. For example, higher incidences of thyroid
cancer have been seen among the survivors of the World War II atom
bombings in Japan, in Pacific islanders accidentally exposed to fallout
after nuclear weapon testing, and in children in Belarus and Ukraine
after the Chernobyl nuclear power plant accident. In addition, 38
million Americans living in states east of Nevada were exposed to
radioactive iodine in fallout from atmospheric nuclear testing between
1952 and 1958. The extent of this risk in people older than 50 years is
uncertain, but can be estimated based on certain personal
characteristics at:http://ntsi131.nci.nih.gov/.
How Does Thyroid Cancer Present?
Most patients with thyroid cancer have no symptoms (i.e., complaints) at all; in some, signs (objective exam findings) can be subtle and easily overlooked. Thyroid cancer is often first detected when an affected person, their doctor, or someone else notices that they have a swelling beneath their Adam’s apple in the front of the neck. Thyroid lumps large enough to see and feel, called palpable nodules, are relatively common, occurring in 6% of adult women and 2% of adult men. Many more thyroid nodules, however, are too small to feel. Careful inspection of the thyroid by sonography, for example, reveals that up to one-third of adult women and one-fifth of men have small nodules in their glands. Such small nodules are discovered when a person has a medical imaging procedure performed for some other reason, such as a sonogram of the carotid arteries; a CAT or MRI scan of their neck, head, or chest; or a PET scan. These very small, incidentally detected thyroid nodules are called thyroid incidentalomas. Fortunately, the vast majority of both palpable and smaller nodules are benign (not cancer), but the possibility of cancer must be considered whenever they are found.
When
a thyroid cancer grows to the extent that it stretches the capsule
around the gland, presses on or invades nearby structures, or spreads to
lymph nodes or other organs outside of the thyroid, then symptoms may
appear. Some patients with thyroid cancer may feel a lump, tightness, or
pain in the front of the neck. Pain from the thyroid gland can
sometimes seem to be coming from the jaw, ear, or throat. Pressure on or
invasion of the windpipe (trachea) can cause cough, coughing up blood, and shortness of breath. Growth surrounding or invading the swallowing tube (esophagus) can produce difficulty swallowing or pain with swallowing. The nerves that control the vocal cords (recurrent laryngeal nerves)
run right behind the thyroid gland, so pressure on or invasion of them
by tumor can cause hoarseness, difficulty swallowing liquids, and
shortness of breath.
Sometimes, the first evidence that a person has thyroid cancer arises from disease spread (metastasis)
that has already occurred. Some people, especially affected children,
present with an enlarged lymph node or multiple nodes in the neck. Other
patients come to the doctor with new and persistent bone pain
reflecting the presence of a metastasis to the skeleton. Spread to lungs
can present with chest pain, coughing up blood, or shortness of breath.
When there is pressure on the spinal cord from a thyroid cancer
metastasis, a person could have weakness or numbness of an extremity, or
difficulty with control of urination or bowel movements. In all of
these circumstances, the presence of thyroid cancer is often not
established until the offending metastasis has been biopsied and found
to be comprised of cells from the thyroid gland.
It is important to remember that most people who have any one of the symptoms noted above do not
have thyroid cancer. Hoarseness, coughing, chest and skeletal pain, and
enlarged lymph nodes in the neck are much more likely to be due to
something else. However, when a symptom or sign, such as those noted
above, is new for that person, has no other obvious explanation (e.g., a
cold), lasts two weeks, or is getting worse, the affected individual
should seek medical attention.
How is Thyroid Cancer Diagnosed?
Thyroid cancer is usually diagnosed in the course of evaluating patients with a thyroid nodule or, less commonly, diffuse gland enlargement (goiter) that has been either palpated (felt) or identified on an imaging study performed for another reason. (See Knol on Goiter and Thyroid Nodules.) Although more than 90% of thyroid nodules are benign tumors or cysts—not cancers—malignancy should, nonetheless, be considered in every affected person by, at least, determining certain key facts from a careful medical history and physical examination. Often patients with small thyroid nodules, less than one cm in diameter, and no risk factors for thyroid cancer can then simply be reexamined or imaged by sonography to be sure the nodule is not enlarging. For larger nodules, additional studies are usually indicated, as described below.
The
clinical evaluation, knows as a history and physical examination, for
patients with one or more thyroid nodules or a goiter collects facts
about potential risk factors for developing thyroid cancer, local neck
symptoms, complaints suggesting metastatic disease, features of
hyperthyroidism or hypothyroidism, and the presence of diseases
associated with thyroid cancer (Table 2). Particularly important facts
from this history include child neck radiation exposure, gland or nodule
enlargement over a few weeks or months, gland pain, persistent
hoarseness or cough, coughing up blood, difficulty swallowing, or a
family history of thyroid cancer or related illnesses. On examination,
worrisome findings include a hard nodule or entire gland that does not
move freely with swallowing and is associated with lymph node
enlargement in the neck.
The history and examination on
their own rarely establish the presence or absence of thyroid cancer, so
additional tests are usually needed. (Figure 3) A thyroid sonogram, in
which inaudible sound waves are beamed into the neck and the returning
echoes depict thyroid and surround tissues, can confirm that a lump in
the neck is actually in the thyroid gland, show whether it is cystic or
solid, and precisely measure its size. Sometimes, sonographic features
of a thyroid nodule make it more suspicious for cancer (e.g., fine
calcium deposits, a rough border, and abnormal lymph nodes nearby in the
neck) or, alternatively, make it less likely to be malignant (e.g., a
small purely fluid-filled cyst). A blood test for TSH is useful in
evaluating people with a thyroid nodule because, if the TSH is low, the
person may have a benign, but hyperfunctioning thyroid tumor, called a
toxic adenoma. The next step in evaluation is a radionuclide thyroid
scan to see if the gland enlargement is, in fact, a “hot” nodule.
However, if the blood TSH level is now low, then people with a thyroid
nodule larger than 1.0 to 1.5 cm (1/2 inch) in diameter, as well as
those with any other features suspicious for cancer, need to have a fine
needle aspiration biopsy to obtain thyroid cells for evaluation by an
expert cytopathologist. A blood calcitonin level may also be checked if
there is any reason to suspect that the patient or a family member has
medullary thyroid cancer due to symptoms associated with high calcitonin
or of other medical conditions known to be associated with this
particular thyroid cancer type (see Table 2). Other special testing for
medullary thyroid cancer is discussed in the section dedicated to that
tumor type below.
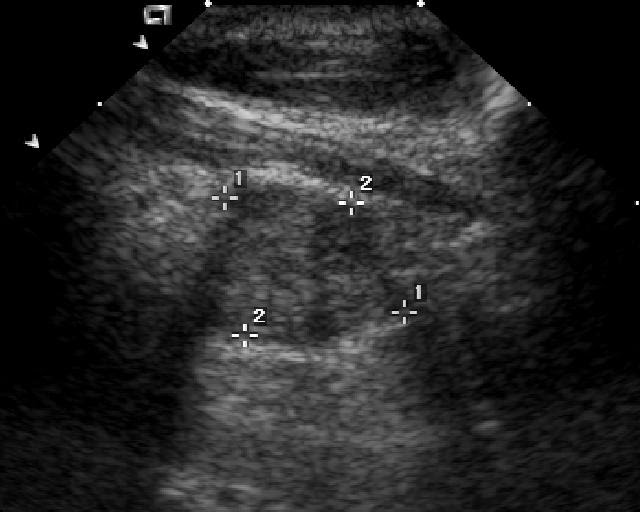

Figure 3. Typical diagnostic testing for a person with a thyroid nodule (Sonographic Features of Thyroid Nodules)
The
test needed to sort out most thyroid nodules is the fine needle
aspiration biopsy, a simply outpatient procedure performed with the
patient wide awake. A physician uses a small needle to withdraw
representative thyroid cells from the nodule, usually guided by an
ultrasound machine to show the location of the nodule during the
procedure. The microscopic examination of cells acquired then leads to
the categorization of nodules into four categories. (Figure 4) First,
the specimen may be inadequate with insufficient thyroid tissue to make a
diagnosis; people with this finding need another biopsy. Second, and
fortunately, most often, the biopsy report is benign. People whose
nodule falls into this category seldom need surgery and can be seen by
their doctor periodically to sure their goiter or nodule is not
progressively enlarging. Third, the biopsy can strongly suggest the
presence of thyroid cancer. When the biopsy findings are interpreted as
malignant, 95% of the time, the person actually proves to have thyroid
cancer at subsequent surgery, so an operation is indicated (unless the
individual has other serious medical problems). The fourth category of
thyroid biopsy finding is uncertain or indeterminate. One in five
biopsies fall into this group, if features of the cells seen are simply
not characteristic enough of a benign or malignant nodule for the
cytopathologist to be sure

Specific Types of Thyroid Cancer (Table 1)
Thyroid Cancer Type
|
Incidence
|
Affected
Family Member(s) |
Typical Management
|
Comments
|
Papillary
|
10%
|
Surgery to remove both sides of thyroid gland (bilateral thyroidectomy)
After surgery, sometimes radioactive iodine to ablate remaining thyroid tissue and treat metastases
Lifelong thyroid hormone medication to replace gland function and suppress pituitary TSH
|
Usually low-grade cancer that is curable
Spread is by extension into neck tissues or metastasis to lymph nodes and/or lung
Mortality is rare, but recurrence is common (1/4 cases)
| |
Follicular
|
<1%
|
Bilateral thyroidectomy, although unilateral thyroid lobectomy may be sufficient for minimally invasive tumors
Postoperative
radioactive iodine for vascular invasive tumors to ablate remaining
normal thyroid and treat iodine-concentrating metastases
Lifelong thyroid hormone medication to replace gland function and suppress pituitary TSH
|
Minimally invasive follicular cancers (i.e., capsular invasion only) behave like low-grade papillary cancer
Vascular invasive follicular cancers can spread in blood to lung, bone, and other sites
| |
Hürthle cell
|
None
|
Same as follicular thyroid cancer, except that the tumor rarely concentrates radioactive iodine
|
Behaves like follicular thyroid cancer
Usually does not concentrate radioactive iodine used for scan detection or treatment
|
Medullary
|
50%
|
Bilateral thyroidectomy, especially for individuals with related familial syndromes
Lifelong thyroid hormone medication to replace gland function, but no need for TSH suppression
|
Tumor arising from parafollicular or C cells, which produce calcitonin
May
occur as familial medullary thyroid cancer or as a component of
multiple endocrine neoplasia syndrome II, along with adrenal and
parathyroid gland tumors
| |
Anaplastic
|
None
|
Surgical removal of the tumor is rarely possible, so limited to biopsy for diagnosis and relief of airway obstruction
Combined chemotherapy and radiation therapy
|
Usually presents in older persons
Very aggressive cancer with rapid growth and early spread to other parts of the body
Extremely difficult to treat
|
Papillary thyroid cancer,
which accounts for 80-90% of all thyroid malignancies, most commonly
arises in adults, but it is also the most common type of thyroid cancer
in older children and adolescents. The name papillary refers to
the fern leaf-like organization of the cells. The nuclei of papillary
thyroid cells have atypical features that often permit diagnosis to be
made by biopsy before surgery. This kind of thyroid cancer has been
associated with mutations in genes that define the structure of proteins
normally involved in thyroid cell growth and proliferations, for
example, Ret, Ras, and BRAF. Papillary cancer
affects another family member in 10% of affected people. In a minority
of individuals with papillary cancer, the tumor is one aspect of an
inherited syndrome with other features, such as colon polyps in
Gardner’s syndrome; skin and mouth lining lumps in Cowden’s syndrome; or
kidney cancer, moles, and lung blebs in Birt-Hogg-Dube syndrome.
The
majority of papillary thyroid cancers remain confined to the thyroid
gland when they are diagnosed, but separate tumors are found in other
parts of the gland in 40% of cases, so called multifocality.
Papillary cancer can spread beyond the thyroid gland by direct growth
into nearby tissues or by traveling through lymphatic or blood vessels
to distant sites. Involvement of lymph nodes in the neck is common,
occurring in one-third of people with the condition. Papillary cancer
can also spread to the lungs and, less commonly, to other parts of the
body. Certain subtypes of papillary thyroid cancer behave more
aggressively, such as tall cell, columnar cell, insular, and poorly
differentiated variants. Treatment of papillary thyroid cancer is
discussed below.
Follicular thyroid cancer, which represents less than 10% of all thyroid malignancies, typically occurs in older adults. Their individual cells look and are oriented in follicles like those in normal thyroid tissue and some benign thyroid tumors. However, when follicular thyroid cancers are removed and examined microscopically, their cells can be seen to penetrate through their surrounding capsule and/or blood vessels within the tumor. Follicular cancers with capsular invasion alone are called minimally invasive. These cancers generally behave like low-grade papillary thyroid cancers and remain confined to the gland. Follicular thyroid cancers that also invade blood vessels are called invasive or angioinvasive follicular thyroid cancers; these cancers can spread via blood to lung, bone, and less commonly, other distant organs around the body.
Hürthle cell cancer, accounting for less than 5% of all thyroid cancers, is similar in most respects to follicular thyroid cancer, except that its cells have swollen cytoplasm that are filled with microscopic structures called mitochondria. Hürthle cell cancers can, like follicular tumors, be either minimally invasive or vascular invasive malignancies. The former are usually confined to the thyroid gland; whereas, the latter having the potential for spread to the lungs, bones, and, rarely, other distant sites. Hürthle cell cancers differ in that they rarely concentrate iodine efficiently, making it more difficult to locate and treat metastatic disease.
Medullary thyroid cancer,
representing less than 10% of thyroid cancers, arises from the
thyroid’s parafollicular C cells, which make calcitonin. Medullary
thyroid cancers are evenly divided between those that affect a single
individual, so called sporadic medullary thyroid cancer, and those that occur as a component of several different inherited familial medullary thyroid cancer syndromes. Medullary thyroid cancers are closely linked to a set of genetic derangements in the Ret
gene, which can unleash cancerous growth of C cells in the thyroid as
well as tumors in other adrenal and parathyroid cell types. Inherited
forms of thyroid C cell cancers include familial medullary cancer alone
and the multiple endocrine neoplasia II (MENII) syndromes. MEN IIa is
comprised of medullary thyroid cancer; pheochromocytoma, a tumor of the
central part of the adrenal (medulla) secreting the ‘fight or flight’
hormones (e.g., epinephrine) that cause high blood pressure that is
often severe, unstable, and hard to control; and parathyroid tumors that
make an excess of parathyroid hormone causing high blood calcium and
related symptoms, kidneys stones, and bone mineral loss. MEN IIb
includes medullary thyroid cancer; pheochromocytoma, and characteristic
benign tumors beneath the mucosa of the mouth and eyelids along with a
lanky body build.
The behavior of
medullary thyroid cancers ranges from incidentally detected microscopic
tumors detected then the thyroid is removed for another reason to
aggressive widely metastatic cancer with symptoms related to both sites
of disease and excess calcitonin production (see above). The state of a
patient’s disease can be monitored with the blood calcitonin level;
another substance called carcinoembryonic antigen (CEA) can also be
useful in monitoring.
In people with an affected family member, tests to analyze the DNA comprising the Ret
gene can identify most of those with risk of developing medullary
thyroid cancer. Blood testing for calcitonin, especially after calcium
stimulation, can also be useful in testing potentially affected
relatives of a medullary thyroid cancer patient. Based on the results of
such testing, young family members with high risk of future disease may
be well advised to have their thyroid removed before the cancer
develops, spreads, and becomes incurable.
Anaplastic thyroid cancer is a high-grade malignancy arising from thyroid tissue that grows rapidly and spreads aggressively to both adjacent structures in the neck and distant sites in the body. Anaplastic thyroid cancers are often impossible to remove surgically. Their cells lose the microscopic and functional characteristics of normal thyroid cells, and as a result, they do not concentrate iodine or respond to radioactive iodine treatment. The prospects have been pretty dismal for people with this condition unless their disease is detected very early and treated aggressively with combined chemotherapy and external beam radiation. New drugs may offer hope for some individuals with this previously incurable form of cancer.
Rarer forms of thyroid malignancy. The thyroid cancer can sometimes give rise to or become involved with tumors of the lymph system, called thyroid lymphomas.
Unlike other forms of thyroid cancer that are usually treated
surgically, thyroid lymphomas can sometimes be effectively treated with a
combination of chemotherapy and radiation. Squamous cell cancers,
like those affecting the upper airway, can also develop in the thyroid
gland. Sometimes cancers that originate from malignancies in other parts
of the body—kidney, colon, lung, and breast—can secondarily spread to
the thyroid.
Table 2. Key Facts in a Patient with a Thyroid Nodule
History
Age and gender
Pattern of gland enlargement
Local neck symptoms
Pain or tenderness of the thyroid
Pain or tenderness of the thyroid
Persistent cough or hoarseness
Coughing up blood
Difficulty or pain with swallowing
Shortness of breath
Swelling of lymph nodes in the neck
Symptoms potentially due to thyroid cancer spread
Bone pain
Chest pain
Weakness or numbness or an arm or leg
Symptoms potentially due to of too much or too little thyroid hormone
Hyperthyroidism:
weight loss, heat intolerance, tremor, palpitations, insomnia, anxiety,
nervousness, increased bowel movement frequency, anxiety, and muscle
weakness
Hypothyroidism: weight
gain, cold intolerance, constipation, dry skin and hair, slowed
thinking, depressed mood, and muscle cramps
Symptoms potentially due to a high calcitonin level in blood: diarrhea, flushing, or itching
Past history of childhood neck irradiation
Past illnesses potentially associated with thyroid cancer (as in Family History below)
Family history of thyroid disease or related illnesses
Benign goiter or thyroid nodules
Thyroid cancer
Thyroid cancer
Colon polyps
Kidney stones, high blood calcium level, or parathyroid gland tumor
Severe high blood pressure or adrenal gland tumor
Physical Examination
Nodule or goiter
Size
Consistency (hard, rubbery, fluctuant)
Tender
Mobility, i.e., move freely with swallowing
Lymph node enlargement in the neck
Signs suggesting an overactive or underactive thyroid gland
Hyperthyroidism: fast heart rate, jitteriness, trembling hands, pounding heart, warm moist skin, muscle weakness
Hypothyroidism: slow heart rate, lethargic, puffy tissues, dry skin and hair, slowed speech and thinking
Signs suggesting features of conditions associated with thyroid cancer
High blood pressure
Lumps beneath the mucosal linings of the lips and eyelids
Tall lanky body build with loose jointedness
How is Thyroid Cancer Treated? (Figure 5)
Thyroid surgery is the initial treatment for most people with known or suspected thyroid cancer to remove either all or only one side of the thyroid gland. When the diagnosis of thyroid cancer has already been established by a biopsy, the preferred operation is bilateral thyroidectomy. This removes other sites of thyroid cancer that are often present in patients with the most common form, papillary thyroid cancer, and it prepares the patient for eradication of any small thyroid tissue remnant with postoperative radioactive iodine. On the other hand, removal of a single thyroid lobe is sometimes preferable, in patients with an indeterminate biopsy because the majority of these patients will not, in fact, prove to have thyroid cancer and will not thereafter have to take thyroid hormone medication.
Thyroid surgery requires general
anesthesia and hospitalization. All patients have some postoperative
discomfort and a small scar in the front of the neck. Injury to nearby
structures occurs in a small percentage (2-10 %) of patients. Such
injury may include damage to the recurrent laryngeal nerves causing
permanent hoarseness, difficulty swallowing fluids, and even trouble
breathing, or removal or other injury to the adjacent parathyroid
glands, causing a low blood calcium level and related symptoms of
tingling, numbness, or muscle cramps requiring prolonged calcium and
vitamin D medications.
Surgery is also used to remove lymph nodes
containing thyroid cancer tissue, either at the time of initial
thyroidectomy or later when remaining thyroid cancer tissue is detected
during the course of long-term monitoring.
Radioactive iodine
is recommended after surgery for some patients with differentiated
thyroid cancers (i.e., papillary, follicular, and Hürthle cell cancers)
to ablate (destroy) the small amount of thyroid tissue that remains in
most patients after thyroidectomy. The two reasons for this treatment
are that 1) patients who initially have more advanced disease are known
to have fewer recurrences of cancer if radioactive iodine is used after
surgery; and 2) the tests used to monitor patients with previously
treated thyroid cancer—blood thyroglobulin levels and radioactive iodine
scans—are most accurate once all normal thyroid tissue has been
completely removed. This additional treatment is usually advisable for
patients who are older with larger tumors that have spread beyond the
gland, have not been completely removed surgically, or have other
microscopic features that suggest they are more aggressive. Tests of
tumor tissue for molecular mutations, such as in BRAF, can also
predict greater risk of recurrence and, some believe, the need for
radioactive iodine treatment. Radioactive iodine is also used to treat
metastatic disease that still can concentrate iodine, a characteristic
that is often retained by follicular thyroid cancers and papillary
thyroid cancers in younger people.
Radioactive iodine is a
relatively simple treatment administered by mouth as a capsule or
liquid; this is usually done without hospitalization in the U.S. Side
effects include inflammation of the salivary and lacrimal (tear) glands,
causing short-term swelling and mild pain, and rarely, long-term dry
mouth or eye, respectively. In order to stimulate radioactive iodine
uptake by thyroid tissue, the blood level of TSH must be elevated. There
are two ways to accomplish this: 1) stopping thyroid hormone medication
so the patient’s own thyroid makes more TSH, or 2) giving genetically
engineered recombinant human TSH as injections to patients who remain on
uninterrupted thyroid hormone treatment. The latter approach avoids
symptoms related to thyroid hormone deficiency (hypothyroidism), which
otherwise occur.
Thyroid hormone medication, L-thyroxine (T4), is an essential part of long-term treatment for patients with thyroid cancer. It replaces the function of their missing gland, ensuring that they will not suffer symptoms and complications of hypothyroidism. L-thyroxine also feeds back on the pituitary gland, suppressing its production of TSH, which might otherwise promote regrowth of thyroid cancer tissue.
Other thyroid cancer treatments may be required for people with more extensive and poorly differentiated thyroid malignancies that cannot be removed surgically or radiated with radioactive iodine.
External beam radiation may be administered to control remaining cancer in the neck that cannot be removed surgically or metastatic disease causing bone pain or pressure on adjacent structures.
Chemotherapy for thyroid cancer, which previously had limited effectiveness and many serious side effects, has recently advanced with the introduction of new agents, called tyrosine kinase inhibitors, which more directly target thyroid cancer cells with greater likelihood of stabilizing disease, and less risk of injury to other body tissues.
How are thyroid cancer patients monitored after initial treatment?
In the past, thyroid cancers had a reputation for recurring even many years after apparent cure. Recent improvements in the techniques for monitoring patients after primary treatment permit the earlier detection of residual disease and its retreatment. Foremost among these tests is measurement of tumor markers in blood: thyroglobulin for differentiated thyroid cancers (papillary, follicular, and Hürthle cell cancers) and calcitonin and CEA for medullary thyroid cancers. For example, after complete thyroid removal with surgery and radioactive iodine, there should be no thyroglobulin remaining in the blood of a treated papillary thyroid cancer patient. For differentiated thyroid cancers capable of concentrating iodine, radioactive iodine scanning can also be helpful in identifying and locating residual disease. Unfortunately, many thyroid cancers lose the ability to capture iodine and be seen or treated. TSH stimulation improves the accuracy of both thyroglobulin blood testing and radioactive iodine scanning, and recombinant TSH administration achieves this without causing the patient to suffer a period of thyroid hormone deficiency.
Radiological imaging techniques can also
help identify residual thyroid cancer after initial treatment.
Sonography of the neck is especially useful to find remaining cancer
tissue in the thyroid bed or lymph nodes in the neck. CT, MR, and PET
scanning all have roles to play in locating residual thyroid cancer
tissue when it persists. When potential sites of remaining disease are
identified by these techniques, the present of thyroid cancer can often
be confirmed by biopsy. Repeat surgery may then be recommended to remove
residual cancer tissue if this is feasible.
Most patients with thyroid cancer enjoy lives that are, otherwise, as healthy and long as anyone else. Their
anxiety about having cancer, their pain after surgery and other
symptoms related to treatments, and the inconvenience and expense
typically fade into the background for most people with the condition. For some, however, more aggressive thyroid cancer is not completely cured after initial treatment. Their condition may require close medical follow-up to detect, locate, and treat residual disease. For a less than 5% of thyroid cancer patients, their disease is currently incurable and life-threatening. For them, recent advances in chemotherapy hold great promise of halting their disease’s progression.
MORE INFORMATION ABOUT THYROID CANCER
Web Resources
American Thyroid Association
Thyroid Nodules: http://www.thyroid.org/patients/patient_brochures/nodules.html
Thyroid Surgery: http://www.thyroid.org/patients/patient_brochures/surgery.html
Radioactive Iodine Use for Thyroid Diseases:
http://www.thyroid.org/patients/patient_brochures/radioactive.html
http://www.thyroid.org/patients/patient_brochures/radioactive.html
Up to Date Patient Information:
http://patients.uptodate.com/indexResults.asp?index=41887&title=Thyroid%20cancer
http://patients.uptodate.com/indexResults.asp?index=41887&title=Thyroid%20cancer
Medline Plus: http://www.nlm.nih.gov/medlineplus/
National Cancer Institute: http://www.cancer.gov/cancertopics/wyntk/thyroid
Books
Quick FACTS Thyroid Cancer. American Cancer Society, 2008
Thyroid Cancer: A Guide for Patients. D. Van Nostrand, 2004 (also
available in Spanish as: Cancer de Tiroides: Guia Para Pacientes.)
The Thyroid Cancer Book. M.S. Rosenthal, 2006
Patient Support Organizations
Thyroid Foundation of America, Inc.One Longfellow Place Suite 1518
Boston , MA 02114
phone (toll-free) 800 832-8321
phone 617 534-1500
fax 617 534-1515
e-mail info@allthyroid.org
www.allthyroid.org
Cutting Edge Thyroiditis Research
Clinical trials in progress: http://www.clinicaltrials.gov/ct2/results?term=Thyroid Cancer
References
Sherman SI. Thyroid carcinoma. Lancet. 2003;361(9356):501-11. PMID: 12583960
Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA. 2006;295:2164-7. PMID: 16684987
Cooper DS, Doherty GM, Haugen BR, et al.; The American Thyroid Association Guidelines Taskforce. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2006;16:109-42. PMID: 16420177
AACE/AME Task Force on Thyroid Nodules. American Association of Clinical Endocrinologists and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr Pract. 2006;12:63-102. PMID: 16596732
Mazzaferri EL, Kloos RT. Clinical review 128: Current approaches to primary therapy for papillary and follicular thyroid cancer. J Clin Endocrinol Metab. 2001;86:1447-63. PMID: 11297567
Jonklaas J, Sarlis NJ, Litofsky D, et al.. Outcomes of patients with differentiated thyroid carcinoma following initial therapy. Thyroid 2006;16:1229-1242.
Sawka AM, Thephamongkhol K, Brouwers M, Thabane L, Browman G, Gerstein HC.
Clinical review 170: A systematic review and metaanalysis of the effectiveness of radioactive iodine remnant ablation for well-differentiated thyroid cancer. J Clin Endocrinol Metab. 2004;89:3668-76. PMID: 15292285
Pacini F, Ladenson PW, Schlumberger M, et al. Radioiodine ablation of thyroid remnants after preparation with recombinant human thyrotropin in differentiated thyroid carcinoma: results of an international, randomized, controlled study. J Clin Endocrinol Metab 2006;91:926-32
Mazzaferri EL, Robbins RJ, Spencer CA, et al. A consensus report of the role of serum thyroglobulin as a monitoring method for low-risk patients with papillary thyroid carcinoma. J Clin Endocrinol Metab. 2003;88:1433-41. PMID: 12679418
Torlontano M, Crocetti U, Augello G, et al. Comparative evaluation of recombinant human thyrotropin-stimulated thyroglobulin levels, 131I whole-body scintigraphy, and neck ultrasonography in the follow-up of patients with papillary thyroid microcarcinoma who have not undergone radioiodine therapy. J Clin Endocrinol Metab. 2006;91:60-3. PMID: 16219716
Brandi ML, Gagel RF, Angeli A, et al. Guidelines for diagnosis and therapy of MEN type 1 and type 2. J Clin Endocrinol Metab. 2001;86:5658-71. PMID: 11739416
Cornett WR, Sharma AK, Day TA, Richardson MS, Hoda RS, van Heerden JA, Fernandes JK. Anaplastic thyroid carcinoma: an overview. Curr Oncol Rep. 2007 Mar;9(2):152-8.