 Author: Dr H. Hunter Handsfield Clinical Professor of Medicine University of Washington 2008-07-28
Author: Dr H. Hunter Handsfield Clinical Professor of Medicine University of Washington 2008-07-28Thursday, March 8, 2012
Gonorrhea
Author: Dr H. Hunter Handsfield Clinical Professor of Medicine University of Washington 2008-07-28The primary sites of infection are the urethra in men and the uterine cervix in women. Infections of the rectum, acquired primarily through receptive anal intercourse, and infections of the throat, acquired primarily by penile-oral contact (fellatio), also are common in women and men who have sex with men (MSM). As is true for most STDs, gonorrhea presents the greatest health threat in women, primarily through infection of the Fallopian tubes, called pelvic inflammatory disease (PID), the most common complication. PID in turn often scars the Fallopian tubes, making gonorrhea a common cause of female infertility and ectopic (tubal) pregnancy. Uncommon complications include urethral stricture (abnormal narrowing of the urethra) in men; acute testicular infection (epididymitis); disseminated gonococcal infection (DGI), in which the infection invades the bloodstream and causes a form of arthritis; and infection of the eyes of babies born to infected mothers, at one time the most common cause of blindness in much of the world. As for all STDs associated with genital inflammation, gonorrhea enhances susceptibility and transmission of human immunodeficiency virus (HIV), contributing to the worldwide AIDS pandemic.
This Knol addresses gonorrhea in adults. The information on frequency, risk factors, and populations at risk reflects the epidemic in the United States and is largely applicable to industrialized countries. Reliable epidemiologic data are lacking in most developing countries, but it is clear that the incidence, prevalence, and frequency of complications tend to be substantially higher than in the United States, with the exception of some predominantly Islamic countries. The information in this article on symptoms, complications, treatment, and the principles of prevention applies to all geographic areas.
HOW COMMON IS GONORRHEA AND WHO IS AT RISK?
Frequency
">In the United States and many industrialized countries, gonorrhea cases are routinely reported to health authorities, such as state or local health departments. The Centers for Disease Control and Prevention (CDC) summarize the annual data. Reported data, however, are incomplete; many cases are not diagnosed and others are not reported or counted. Therefore special research efforts, extrapolation from limited epidemiologic analyses, and often creative interpretation of the data are needed to estimate the actual infection rates. The incidence of a disease is the number of cases occurring over a particular time, such as infections per year). Prevalence is the number of cases that exist at any particular moment, such as the percent of the population carrying the infection. Both measures are used to estimate the frequency of gonorrhea and other STDs.
This
graph shows the incidence of reported gonorrhea in the United States
since the early 1940s, when reliable statistics first became available.
The reported rates since the 1970s are more accurate than the earlier
figures, because diagnostic tests have improved and testing is more
widespread than in past years. For example, it is likely that the true
incidence in the early 1940s was at least as high as in the 1970s. The
rates of STD always rise in wartime and other times of societal stress
and disruption. The opposite effects of World War II and the post-war
economic gains on gonorrhea are apparent in the figure, as is the
dramatic rise associated with the sexual maturation (if not yet the
emotional maturation) of the baby boom generation. The rapid decline
after the 1970s was largely due to national prevention strategies
promoted by CDC. (Prior to the 1970s, almost all public funding for STD
prevention was directed toward syphilis.) The incidence of gonorrhea
has been more or less stable for a decade, with annual incidences of
reported infections from 115 to 121 cases per 100,000 members of the
population from 1996 through 2006. However, the incidence rose more
than 5% from 2005 to 2006, the highest proportionate increase since 1973
and a substantial concern to health authorities. After adjusting for
infections that go undiagnosed or not reported to health authorities,
the 358,366 cases reported in 2006 probably reflect about 700,000 actual
cases.

The
rate of gonorrhea in women is slightly higher than in men, reflecting
more frequent testing of women during routine health care visits. This
figure shows the rates in 2006 by both sex and age. As for all STDs,
there is a strong association of gonorrhea with youth, although this
association is less strong than for chlamydia [link to chlamydia Knol].
The highest rate of reported gonorrhea in 2006, 528 cases per 100,000,
occurred in persons aged 20-24. However, the rate of 308 per 100,000 in
15-19 year old persons translates to over 600 cases per 100,000 if you
only count those teens who were sexually experienced. In other words,
considering only those people who are sexually active, the highest rate
of gonorrhea occurs in teens. In the period 1999-2002, among all United
States residents 14-39 years of age, 0.24% were infected with N. gonorrhoeae,
as measured by urine testing—a minimal figure that does not include
infections of the rectum and throat. This rate translates to
approximately 244,000 [check] persons infected at the time of the
survey. While substantial, this rate is about tenfold lower than for
chlamydial infection.
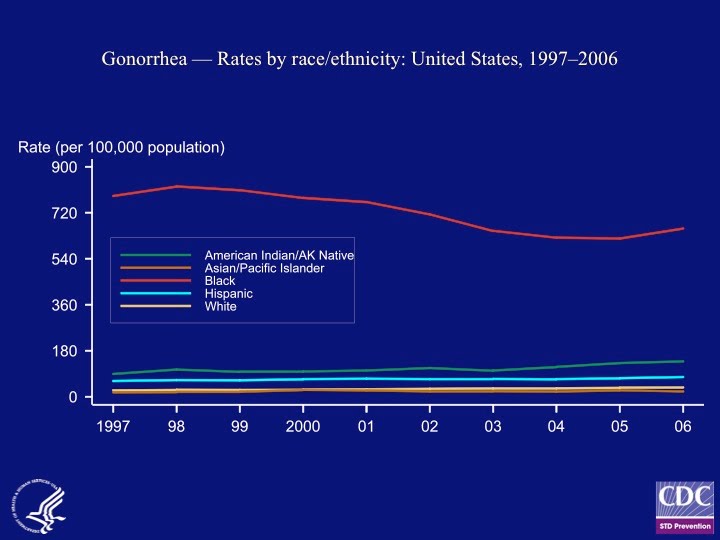
The
dominant demographic predictor of gonorrhea is race, and this figure
displays the reported case rates for 2006 among the dominant
race/ethnicity groupings. The incidence was 18 times higher in African
Americans – and twice as high in persons of Hispanic ancestry – as in
whites. These dramatic differences, especially between African
Americans and other groups, are not primarily due to differences in
sexual activity; indeed, on average African Americans and Hispanics have
no greater numbers of sex partners than whites. Rather, the
explanations lie in population dynamics, the structure of sex partner
networks, family stability, greater attendance by persons of lower
socioeconomic attainment at public clinics where case reporting is most
complete, lower average education, and lesser access to health care,
among other factors.
Finally,
gonorrhea rates vary widely between geographic areas and by
socioeconomic status. For example, in 2006 the highest reported rate,
370 cases per 100,000 in the Memphis metropolitan area, was more than
ten-fold higher than the lowest rate, 35 per 100,000 in Boston.
Comprehensive data are available from CDC [link].
Of
industrialized countries with reliable public health statistics, the
United States has among the highest rates of gonorrhea. The frequencies
in most Western European countries are from 5 to 10 cases per 100,000
annually, more than 10-fold lower than in the United States. These
variances result largely from differences in population subgroups, the
prevalence of social disruptive factors, population mobility, education
level, access to health care, and related issues. For example, most
western European countries offer cost free health care and lack large
minority populations analogous to African Americans and other subgroups
that drive overall incidence. The estimated rates are consistently
highest where social and economic conditions preclude systematic
prevention through screening, case finding, and prompt treatment, and
where war and other societal stresses are maximal, such as most
developing countries and some countries of Eastern Europe.
Transmission
In
adults, gonorrhea is passed from person to person almost exclusively by
sexual activity. Rare non-sexually acquired cases result from such
events as childbirth, which risks infection of the baby if the mother is
infected; laboratory accidents (e.g., exposure of laboratory workers’
eyes through lapses in safe technique); and maybe transmission among
toddlers in conditions of crowding in tropical environments. The common
theme is that N. gonorrhoeae does not survive drying or other
environmental stresses, so that transmission requires the direct
exchange of infected secretions or the direct apposition of moist,
infected surfaces, conditions that in adults are limited to sexual
activity. Insertive penile-vaginal and penile-anal intercourse are the
dominant mechanisms, although penile-oral sex accounts for a substantial
minority of cases. Cunnilingus, i.e. oral contact with female
genitals, is an inefficient mechanism that accounts for infrequent
cases, for which reason gonorrhea is rare in exclusively lesbian women.
Gonorrhea is rarely if ever transmitted by kissing.
Even
for penile insertive intercourse, transmission is not 100% efficient.
The risk of transmission from men with urethral gonorrhea to their
female partners has been estimated at 50% for each episode of
unprotected vaginal sex, and the estimated transmission risk in the
opposite direction is around 20%. Finally, for all STDs, transmission
risk mostly transmitted by infected persons without symptoms, or with
only minor symptoms that do not seem important. This happens because
persons with obvious symptoms, such as abnormal discharge from the penis
or vagina, and those with pain or genital sores, are less likely to be
sexually active than those without such symptoms. Therefore, gonorrhea
and other STDs are selectively transmitted by those without prominent
symptoms. This fact underlies a basic STD prevention principle: the
partners of infected people need to be actively notified and treated,
because those who transmitted the infection to the original patient
often have nothing to warn them they might be infected and do not seek
health care on their own.
WHAT ARE THE SYMPTOMS AND SIGNS OF GONORRHEA?
The
hallmarks of gonorrhea result directly from infection of the urethra in
men, the cervix and sometimes the urethra in women, the rectum of
either men or women, and rarely of the throat, eyes, or other sites.
Urethral Gonorrhea in Men
The
dominant symptom of urethral gonorrhea, technically called gonococcal
urethritis, is abnormal discharge from the penis, typically of yellowish
(pus-like) fluid, sometimes scant, but often in large amount. A
typical case is shown in this photograph. Penile pain or discomfort,
primarily upon urination, also is common. The incubation period – the
interval between infection and first symptoms – usually is three to five
days, occasionally as short as two or as long as 10 days. From 1% to
10% of cases remain asymptomatic and still more have mild symptoms, such
as scant or cloudy rather than overt or yellow discharge. The
proportion of men with symptoms depends in part on specific strains of
N. gonorrhoeae in the community; some strains are more likely than
others to cause less symptomatic infections.
Among
all men with symptoms of urethritis (infection of the urethra), most do
not have gonorrhea; chlamydia and other bacteria, which collectively
cause nongonococcal urethritis (NGU), are more common. The symptoms of
gonorrhea usually are more prominent than those of chlamydia or NGU,
with greater amounts of urethral discharge, a yellow or creamy
appearance, and greater urinary discomfort; compare this photo of NGU
with the gonorrhea image above.
Genital Gonorrhea in Women
The
primary manifestations in women result from infection of the uterine
cervix and, to a lesser extent, the urethra. Up to half of infected
women remain asymptomatic, and when symptoms occur they often are mild
and nonspecific; that is, the symptoms may not be notably different than
day-to-day variations in the amount of vaginal discharge and other
minor genital discomfort. Women who notice gonorrhea symptoms typically
have an incubation period of two to 10 days and usually experience
increased vaginal discharge and sometimes urinary urgency or discomfort
on urination, sometimes mimicking the symptoms of non-sexually
transmitted urinary tract infection. Bleeding between menstrual
periods, sometimes heavy in amount and sometimes triggered by sex, also
is common. More women with gonorrhea than those with chlamydia have
symptoms, and the amount of discharge, pain or bleeding tend to be more
prominent.
Examination
by an experienced clinician may reveal mucopurulent cervicitis (MPC),
indicated by inflammatory signs of the uterine cervix, such as increased
redness or abnormal discharge of mucus or pus from the cervical
opening. MPC is addressed in more detail in the chlamydia Knol [link].
Sometimes the examiner can express abnormal discharge by applying
pressure to the urethra or the ducts of the Bartholin glands (which
provide sexual lubrication and are located on each side of the vaginal
opening). This photo shows "mucopurulent" discharge (pus mixed with mucus) emanating from the cervical opening in a woman with gonorrhea.
Other Localized Infections in Men and Women
Up
to 90% of women with gonorrhea of the cervix also are infected in the
urethra, explaining the high frequency of urinary discomfort in women
with symptoms. The rectum is infected in about 40% of women and MSM
with gonorrhea. Most have no rectal or anal symptoms, but some infected
persons notice discharge of mucus or pus from the anus, pain, itching
and sometimes rectal bleeding, and some persons observe white
exudate—often described by patients as mucus—that coats feces following
bowel movements. Rectal infection in MSM is acquired by anal sex, and
in women both by anal sex and contamination of the anal area by
discharge from the vagina. Gonorrhea of the throat (pharynx) is present
in 5% to 10% of infected women and 10% to 20% of infected MSM,
exclusively in those who perform fellatio on their male partners.
Transmission by cunnilingus is rare, so pharyngeal gonorrhea is uncommon
in exclusively heterosexual men. Most pharyngeal infections are
asymptomatic, but once in a while they cause sore throat, and rarely
severe manifestations that mimic strep throat, with pus visible in the
back of the pharynx or on the tonsils.
Gonococcal
conjunctivitis—infection of the lining of the eyelids—is uncommon. It
can occur through auto-inoculation, as when a person with genital
gonorrhea touches the eyes with contaminated fingers. Mild cases mimic
pink-eye due to common viruses, with itching and minor irritation, but
severe cases can cause prominent redness and discharge of pus, and
without prompt treatment can destroy the cornea, leading to blindness.
Gonococcal conjunctivitis of the newborn (ophthalmia neonatorum) once
was the most common cause of blindness but now is almost completely
prevented by routine testing of pregnant women to detect gonorrhea, and
by routine antibiotic eye drops given to all newborns.
Natural Course of Untreated Gonorrhea
It
is commonly assumed that untreated gonorrhea or other STDs inevitably
persist if not treated with antibiotics. However, the large majority of
bacterial infections of all causes, including gonorrhea, eventually are
controlled by the immune system and resolve without treatment. Before
the development of modern antibiotics, uncomplicated urethral gonorrhea
in men generally resolved within several weeks, although often followed
by scarring that resulted in urethral stricture, with later urinary
obstruction. Infection tends to persist longer in women, but
spontaneous resolution after several weeks or months is the rule, with
or without intervening PID and its consequences. However, rare cases
may persist for several months, sometimes explaining positive diagnostic
tests in women seemingly not at risk for new infection.
Complications
Pelvic Inflammatory Disease.
PID refers to infection of the Fallopian tubes and is the most common
complication of gonorrhea regardless of gender. Chlamydia is the most
common overall cause of PID, but gonorrhea tends to be associated with
more severe symptoms. Either infection often involves other bacteria
from the vagina, so that treatment requires antibiotics active against a
wide range of bacteria in addition to chlamydia and gonorrhea. Up to
half of all PID cases are caused by neither gonorrhea nor chlamydia, and
some are not sexually acquired. Many such cases occur in women with
prior PID, probably because damage to the Fallopian tubes predisposes to
infection with normal vaginal bacteria.
Regardless
of the cause, the hallmark of PID is pain in the lower abdomen.
Infecttion often spills from the Fallopian tubes into the abdominal
cavity, resulting in localized abscesses and sometimes extensive
intra-abdominal infection (peritonitis). A variant of gonococcal or
chlamydial peritonitis is called perihepatitis, or the Fitz-Hugh—Curtis
syndrome; it results when infection is localized around the liver and
can mimic the symptoms of hepatitis or gall bladder disease. Fever is
common in women with PID but not invariably present, and sometimes the
first symptom is pain in the abdomen during intercourse, because
movement of the cervix is often painful in the presence of pelvic
infection. Some women are severely ill with high fever and serious
pain, but others have only mild abdominal discomfort. In addition to
abdominal pain and fever, most women with PID notice abnormal vaginal
discharge.
Pelvic
examination typically reveals tenderness of the uterus, ovaries, and
Fallopian tubes. Without prompt treatment, 10% to 20% of PID results in
blocked the Fallopian tubes, resulting in infertility and an elevated
risk of life-threatening ectopic (tubal) pregnancy. For this reason,
experts recommend treatment for possible PID even when the infection is
merely suspected, without proof of the diagnosis. Ultrasound
examination often is used to document swollen or pus-filled Fallopian
tubes, pelvic abscesses, and other abnormalities caused by PID. PID
sometimes is difficult to distinguish from other causes of
intra-abdominal inflammation, such as endometriosis, internal pelvic
bleeding during ovulation (mittelschmerz), ectopic pregnancy,
appendicitis, diverticulitis, and other conditions.
Epididymitis.
Epididymitis is the male counterpart of PID in women, with infection of
the sperm collecting duct (vas defrens) and into a testicle, resulting
in testicular pain, swelling, and sometimes fever. Epididymitis is a
rare complication of gonorrhea; chlamydia is a much more common cause of
epididymitis. The condition is discussed in more detail in the Knol on
chlamydia. [link]
Disseminated Gonococcal Infection. Some strains of N. gonorrhoeae
are prone to invade the blood stream, resulting in disseminated
gonococcal infection (DGI). DGI is uncommon, occurring in no more than
one percent of infected people, although the actual risk varies from
time to time as particular strains fluctuate in the community. The main
manifestations are arthritis and the arthritis-like condition called
tenosynovitis, with pain and swelling in one or more joints (first
photo), usually with fever. About two thirds of cases include a
characteristic skin rash, with scattered red bumps or pimple-like
lesions (second photo). Infection of a heart valve (endocarditis) is a
rare but potentially fatal complication. DGI is sometimes confused with
reactive arthritis, an occasional complication of chlamydia [link to
chlamydia Knol]. The diagnosis of DGI can be difficult, in part because
the gonococcal strains most likely to cause DGI are the same ones most
likely to cause genital infection without symptoms. Therefore, many
patients with DGI present with joint pain and skin rash, but without
genital symptoms to alert the clinician to the possibility of gonorrhea.


HOW IS GONORRHEA DIAGNOSED?
Gonorrhea
can be suspected by the trained clinician, based on symptoms and
physical examination. However, there is considerable overlap between
gonorrhea and NGU and cervicitis. Therefore, laboratory testing is
required for definitive diagnosis. The main diagnostic method is to
identify N. gonorrhoeae at the site of infection, typically after
collecting a specimen on a swab or by testing urine. No blood test is
available to detect gonorrhea.
Microscopy and Culture

Gonococci
can be readily recognized by examination of infected secretions under a
microscope, after coloring the specimen with the procedure called
Gram’s stain, and Gram stained smears continue in common use for rapid
diagnosis of urethral gonorrhea in men. This drawn figure illustrates
the microscopic appearance of a Gram stained smear from a man with
gonorrhea, with white blood cells packed with pink (“Gram negative”)
kidney-shaped pairs of gonococci.
However, stained smears miss most infections of anatomic sites other
than the male urethra and are not useful for diagnosis of gonorrhea in
women.
Historically,
culture was the preferred method for definitive diagnosis, i.e. to grow
gonococci in the laboratory from specimens collected on swabs from the
urethra, cervix, rectum or throat. For the better part of a century,
the culture and stained smears were the only methods available for
diagnosis, but they miss many infections. Culture remains in wide use,
especially for epidemiologic surveillance, e.g. to evaluate trends in
antibiotic resistance.
Nucleic Acid Amplification Tests
Tn
the past 15 years culture has largely been supplanted by the nucleic
acid amplification tests (NAAT), in which minute quantities of DNA can
be identified in clinical specimens. NAATs are both highly sensitive –
capable of detecting almost all gonococcal infections – and highly
specific, so they avoid false positive results. NAAT methods include
the polymerase chain reaction (PCR), the ligase chain reaction (LCR),
the DNA strand displacement assay (SDA), and transcription mediated
analysis (TMA); gonorrhea tests using each of these technologies are now
the mainstay of diagnosis. Recent research shows that the NAATs also
give reliable results when used to test specimens from the rectum or
throat, making the tests useful in diagnosing gonorrhea in MSM. NAATs
are discussed in more detail in the Knol on chlamydia.
HOW IS GONORRHEA TREATED?
Authorities
such as CDC recommend treatment when gonorrhea is suspected, without
awaiting diagnostic confirmation. For example, treatment is routine
before test results are known for the sex partners of infected persons,
and often for people with urethritis, MPC, proctitis, PID, or
epididymitis even when gonorrhea is much less likely than chlamydia or
other infections. Because 10% to 50% of persons with gonorrhea are
co-infected with chlamydia, treatment of gonorrhea routinely is
accompanied by drugs active against chlamydia. The table lists the
regimens recommended by CDC for treatment of uncomplicated gonorrhea.
http://www.cdc.gov/std/treatment/2006/toc.htm.
Antibiotic Resistance
In
the past decade, the general public has come to understand that
bacteria readily develop resistance to antibiotics. (From the
perspective of the gonococcus and other bacteria, antibiotics represent a
toxin in the environment, and mutants with increased resistance respond
to selection pressure by propagating preferentially, an example of
Darwinian evolution in action.) N. gonorrhoeae was among the
first bacteria to demonstrate this effect. When the sulfa drugs, the
first potent antibiotics, were first used in the 1930s, they were highly
effective against gonorrhea, but within five years sulfa treatment was
useless. When penicillin was introduced in the 1940s, gonorrhea
responded to very low doses, but within two years the dose needed for
reliable cure had doubled. This trend, with steadily increasing doses
required for reliable cure, continues to the present time. In the
1970s, N. gonorrhoeae strains evolved that were resistant to any dose of
penicillin. Increasing resistance has occurred for the tetracycline
class of antibiotics, the aminoglycosides (streptomycin and related
compounds), the macrolides (erythromycin and others) and, most recently,
ciprofloxacin (Cipro®) and other fluoroquinolones, which until the
1990s were a worldwide mainstay of therapy.
At
present, few gonococci are resistant to the cephalosporin class of
antibiotics, such as ceftriaxone (Rocephin®), cefixime (Suprax®) and
others, which retain their activity against gonorrhea and are the
current drugs of choice in the United States and most areas of the
world. However, even the cephalosporins do not enjoy a secure position
as weapons against gonorrhea. Gonococci with significant resistance to
the cephalosporins have begun to evolve in Japan, and it may be only a
matter of time before such strains appear elsewhere. Fortunately,
reduced use of some older antibiotics has been followed by re-emergence
of less resistant gonococci, and newer antibiotics in development may
hold promise. For the moment, adequate treatment at relatively low cost
remains widely available in industrialized countries, but these issues
are critically affecting gonorrhea control in some developing countries,
where the cheapest drugs—e.g., ciprofloxacin—no longer are effective.
Antibiotics
Routine Treatment.
Compared with most bacterial infections, gonorrhea is unusual in that
single dose treatment is effective. This fortunate fact has greatly
helped the control of gonorrhea, because effective treatment does not
depend on the patient remembering to take a drug for several days. The
table summarizes the treatments recommended by CDC in the United States http://www.cdc.gov/std/treatment/2006/toc.htm.
Treatment of Uncomplicated Gonorrhea in Adults
Ceftriaxone (Rocephin®) 125 milligrams by intramuscular injection, single dose
OR
Cefixime (Suprax®) 400 milligrams orally, single dose
AND
Treatment for chlamydia with azithromycin
(Zithromax®) 1 gram orally in a single dose OR
doxycycline (Vibramycin® and others), 100 milligrams orally twice
daily for 7 days (if chlamydia has not been ruled
out by laboratory testing)
NOTES
If neither ceftriaxone not cefixime is available,
substitute cefuroxime (Ceftin®) 1 gram orally OR
cefpodoxime (Vaintin®) 400 mg orally. Only ceftriaxone is recommended
for pharngeal infection. Persons with
documented allergy to the cephalosporins or serious allergic reactions
to penicillin should be treated with spectinomycin
(Trobicin®) 2 grams by intramuscular injection or
with azithromycin (Zithromax®) 2 grams by mouth.
Ceftriaxone
is highly effective against uncomplicated gonorrhea, but carries the
disadvantage of requiring intramuscular injection, disliked by patients
and clinicians alike. The most effective orally administered
cephalosporin antibiotic, cefixime, currently is not available in the
United States, but its reintroduction is anticipated. Cefuroxime
(Ceftin®) and cefpodoxime (Vantin®) have been less well studied; they
appear to be effective for genital or rectal infection, but not for
gonorrhea of the throat. When a cephalosporin cannot be given—for
example, in persons allergic to such drugs—the main options are
spectinomycin (Trobicin®) or azithromycin (Zithromax®) by mouth. In the
recommended doses, both of these are expensive and poorly tolerated. All patients with gonorrhea are routinely treated for chlamydia; the regimens are described in detail in the Knol on chlamydia.
Treatment of Complications.
PID requires prolonged treatment, usually for 10-14 days, with
antibiotics that suppress not only gonorrhea but also chlamydia and many
other bacteria that often co-infect the Fallopian tubes. One example
is the combination of ceftriaxone or another cephalosporin with
doxycycline, often with the addition of metronidazole (Flagyl® and other
brands). Intravenous antibiotics are required for severe cases.
Prolonged therapy, often given intravenously in severe cases, is
required for gonococcal epididymitis or DGI.
Treatment of Sex Partners
Assuring
treatment of partners is the responsibility of the infected person and
the health care provider. Ideally, infected persons’ partners should be
professionally examined and counseled before being treated. However,
when patients are unable or unwilling to contact the partners who they
believe infected them, or when partners cannot be located or contacted
or refuse to seek care despite being informed, treatment is warranted
even without direct examination. This often can be accomplished by
expedited partner treatment (EPT), whereby the clinician provides a
prescriptions or medication for the patient to take to his or her
partner. http://www.cdc.gov/std/treatment/2006/toc.htm
http://www.cdc.gov/std/ept/ EPT is discussed more thoroughly in the Knol
on chlamydia.
Follow-up Testing
Test of Cure.
The recommended treatments for gonorrhea are sufficiently reliable that
routine retesting to assure cure generally is not necessary. However,
test of cure is recommended for infected persons who might be unable to
comply with treatment or if atypical antibiotic regimens are used. Test
of cure should be done three weeks or more after completion of
treatment. Earlier testing risks false positive results, because NAATs
can detect DNA up to two to three weeks after the organism has been
killed, resulting in false positive test results.
Rescreening.
Although routine test of cure is not usually necessary, CDC and other
health agencies now advise “rescreening” in its place--that is, delayed
retesting a few months after treatment. Among men and women with either
gonorrhea or chlamydia, 10% to 20% are found to be infected again when
retested three to six months later. Most cases result from reinfection,
either from an untreated partner or by sex with other partners, but
some cases result from persistent infection despite normally effective
antibiotic treatment. Rescreening is advised for all patients with
gonorrhea or chlamydia, regardless of whether all partners were treated,
whether or not condoms were used for sex following treatment, and
whether or not new sex partners are believed to be at risk.
HOW CAN GONORRHEA BE PREVENTED?
Prevention
and control of STD can be viewed from the perspective of the individual
at risk, who prefers to avoid infection or, if already infected, wants
to prevent complications; and from the perspective of health care
providers and prevention agencies, such as health departments. These
perspectives overlap with one another. For example, health care
providers are advised to routinely test patients at risk for gonorrhea,
but sexually active persons can request testing when the provider does
not take the initiative. Similarly, providers should promote condom
use, but only persons at risk can choose to use them.
Public Health Prevention Strategies
A
mainstay of gonorrhea prevention is laboratory-based screening, i.e.,
routine testing of persons at risk. Dual NAATs that detect both
gonorrhea and chlamydia are in widespread use, so that most persons
tested for chlamydia also receive gonorrhea tests. This approach is
inefficient, because gonorrhea is much less common than chlamydia in
most sexually active populations. Nevertheless, such screening in women
probably contributes significantly to gonorrhea control. Among men,
asymptomatic urethral gonorrhea is too uncommon to justify the expense
of routine testing in most settings. However, asymptomatic rectal and
pharyngeal infections are highly prevalent in most MSM, in whom routine
screening is indicated, especially in men who have had new sex partners
since previously tested.
In
addition to diagnostic screening tests, important gonorrhea prevention
strategies include promulgation and use of recommended treatment
regimens, assuring treatment of infected persons’ sex partners,
counseling and education programs, professional education of health care
providers in clinical management and prevention, and surveillance
through required reporting of infections to local and state health
departments, which in turn permits the efficient targeting of prevention
resources where needed.
Personal Prevention
Prevention
of STDs and HIV is discussed comprehensively in the Knol on Safe Sex.
[link] Consistent use of condoms for vaginal or anal intercourse outside
committed, mutually monogamous relationships is a core prevention
strategy for all STDs and HIV infection. Oral sex is considerably safer
than genital or anal intercourse, but not risk-free. Selection
of partners at low risk, using simple, common-sense guidelines, is
important in preventing gonorrhea and other STDs. A crucial but often
neglected strategy is "do ask, do tell"--i.e., to routinely ask
potential partners if they are likely to be infected and to be aware of
and share one's own infection history.
Sexually
active persons outside mutually monogamous relationships, especially
teens, young adults, and sexually active MSM of all ages, periodically
should seek routine screening tests for gonorrhea, chlamydia, syphilis,
HIV, and sometimes genital herpes. The frequency of recommended
screening depends on risk. Annual testing makes sense for most sexually
active young persons, but some groups at risk — such as MSM with
multiple partners, sexually active teens, and commercial sex workers —
should be tested as often as two to four times per year. Finally, all
sexually active persons should be aware of the common symptoms of STD
and promptly seek care when such health problems appear, either in
themselves or their sex partners.
SUGGESTED READING
1.
Handsfield HH, Sparling PF. Gonococcal Infections. Chapter 322 in
Goldman L, Ausiello D, et al (ed). Cecil Medicine, 23rd edition.
Philadelphia, Saunders, 2007:2217-23. An overview in a standard internal medicine textbook.
2.
Handsfield HH. Gonorrhea. Chapter 3 in Color Atlas and Synopsis of
Sexually Transmitted Diseases, 2nd edition. New York, McGraw-Hill,
2001:22-32. An extensively illustrated review, intended for health professionals but easily understood by all readers.
3.
Datta SD, et al. Gonorrhea and chlamydia in the United States among
Persons 14 to 39 Years of Age, 1999 to 2002. Annals of Internal
Medicine 2007;147:89-96. The report of the most comprehensive national survey of these STDs in the US.
4. CDC. Sexually Transmitted Disease Surveillance, 2006. Atlanta, GA, November 2007. http://www.cdc.gov/std/stats/trends2006.htm Annually updated statistics on reported STD in the US.
5. CDC. Sexually Transmitted Diseases Treatment Guidelines, 2006. Morbidity and Mortality Weekly Report 2006;55:RR-11. http://www.cdc.gov/std/treatment/2006/toc.htm CDC's treatment recommendations, including summaries of key information about all STDs.
6. CDC. Expedited Partner Therapy in the Management of Sexually Transmitted Diseases, 2006. http://www.cdc.gov/std/ept/ CDC's
summary of outcomes of research studies and recommendations use of
streamlined approaches to assure that partners of persons with gonorrhea
or chlamydia receive treatment.
7.
Newman LM, et al. Update on the management of gonorrhea in adults in
the United States. Clinical Infectious Diseases 2007;44:S84-101. A review of the data that support the CDC gonorrhea treatment recommendations.