“The current methods by which we analyze pain in kids are suboptimal,” said senior author Jeannie Huang, MD, MPH, a professor in the UC San Diego School of Medicine Department of Pediatrics and a gastroenterologist at Rady Children’s Hospital-San Diego. “In this study, we developed and tested a new instrument, which allowed us to automatically assess pain in children in a clinical setting. We believe this technology, which enables continuous pain monitoring, can lead to better and more timely pain management.”
The researchers used the software to analyze pain-related facial expressions from video taken of 50 youths, ages five to 18 years old, who had undergone laparoscopic appendectomies at Rady Children’s Hospital-San Diego. Based on the analysis, along with clinical data input by the study team, the software provided pain level scores for each participant.
Huang said controlling pain is important, not only for the child’s comfort, but also for recovery. Studies have shown that under-treatment of pain is associated with adverse surgical outcomes. “Accurate assessment of pain is a fundamental tenet of delivery of care,” she said.
Several issues, particularly age-related communication difficulties, make existing pediatric pain assessment methods problematic, said Huang. “The current gold standard for measuring pain is self-reporting,” she said, noting patients are generally asked to rate their pain on a scale of zero to 10. “But in pediatrics there is a limited population of kids who can answer that question in a meaningful way. Younger children can have difficulty - a two-year-old hasn’t developed the cognitive and conceptual abilities to think in those terms.”
Clinical pain assessments, aided by nurses or parents, are often used in lieu of patient self-report in children because of these limitations. However, several previous studies have shown nursing staff may have difficulty accurately estimating pain (often underestimating pain), particularly among pediatric patients. Parents are generally more in tune with their children’s pain levels, but may not always be available, said Huang.
Another problem with pain assessment protocols, Huang added, is that pain checks tend to be scheduled and consequently may not coincide with times when pain occurs and when intervention is needed. “Pain assessments are typically scheduled along with vital signs, the frequency of which can vary from every 4 to 8 hours depending on patient severity.”
In the study, researchers filmed the participants at three different visits post-surgery: within 24 hours after an appendectomy; one calendar day after the first visit and at a follow-up visit 2 to 4 weeks after surgery. Facial video recordings and self-reported pain ratings by the participant and pain ratings by parents and nurses were collected.
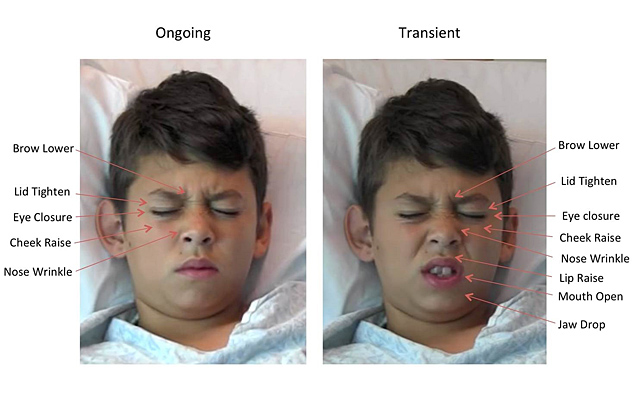
The research team sought to determine the software’s accuracy at pain measurement as compared to self-reporting by the child and as compared to by proxy estimations by parents and nurses. The software prototype utilized data collected via prior software (Computer Expression Recognition Toolbox) by study co-author Marian Bartlett, PhD, at UC San Diego’s Institute for Neural Computation, which utilizes computer vision techniques to analyze facial expressions based on the Facial Action Coding System (FACS). FACS measures facial expressions using 46 anatomically based component movements and has been used in many studies by Kenneth Craig, PhD, a professor of psychology at the University of British Columbia, a world renowned pain expert, and one of the study’s co-authors.
The use of FACS in the past has allowed for identification of pain-related facial movements, but this project took facial movement and pain analysis one step further. In the software prototype, the study’s authors translated the facial movement data into a pain score and then compared that with the information collected from the child’s self-reporting and the parent and nurse by proxy pain estimations.
“The software demonstrated good-to-excellent accuracy in assessing pain conditions,” said Huang. “Overall, this technology performed equivalent to parents and better than nurses. It also showed strong correlations with patient self-reported pain ratings.” The software also did not demonstrate bias in pain assessment by ethnicity, race, gender, or age in the patient cohort studied.
Since the instrument is capable of “operating in real-time and continuously,” using this approach to alert clinicians to instances of pain at the time they occur instead of during scheduled assessments might enhance efficient, timely allocation of pain interventions, noted Huang. Furthermore, such technology could potentially advocate for youth in pain when their parents are unavailable to notify medical staff regarding their child’s pain level.
Huang said the approach requires further investigation with other forms of clinical pain and across the broad age range of children. “It still needs to be determined whether such a tool can be easily integrated into clinical workflow and thus add benefit to current clinical pain assessment methods and ultimately treatment paradigms,” she said.
Coauthors include Karan Sikka, Alex Ahmed, and Damaris Diaz, UCSD; and Matthew Goodwin, Northeastern University.